This article describes evidence-based clinical conventions used in TRT prescribing and androgen monitoring. It is not medical advice. Diagnosis and treatment decisions on TRT require evaluation by a licensed prescriber.
Key Takeaways
DHT is the most potent androgen the body produces -- 3-5x more receptor-active than testosterone
TRT raises DHT 2-3x with injections and substantially more with scrotal cream
DHT is a situational lab, not a routine one -- order it when a specific symptom appears, not at every check
Delivery method, injection frequency, and dose drive DHT more than total weekly milligrams alone
Finasteride and dutasteride lower DHT but introduce their own side-effect ledger
Anti-overcorrection rule: do not blanket-lower DHT in a symptom-free man -- it is doing useful work
If you ask ten TRT prescribers whether to test DHT, you will get ten different answers. Some run it at every follow-up. Some never order it. Most sit somewhere in the middle and check it only when a man walks in with a specific complaint that points at the androgen pathway.
This guide is the middle position with structure -- when DHT belongs on the panel, when the number changes the protocol, and the order of operations for lowering it when symptoms make that the right move.
What DHT Actually Is
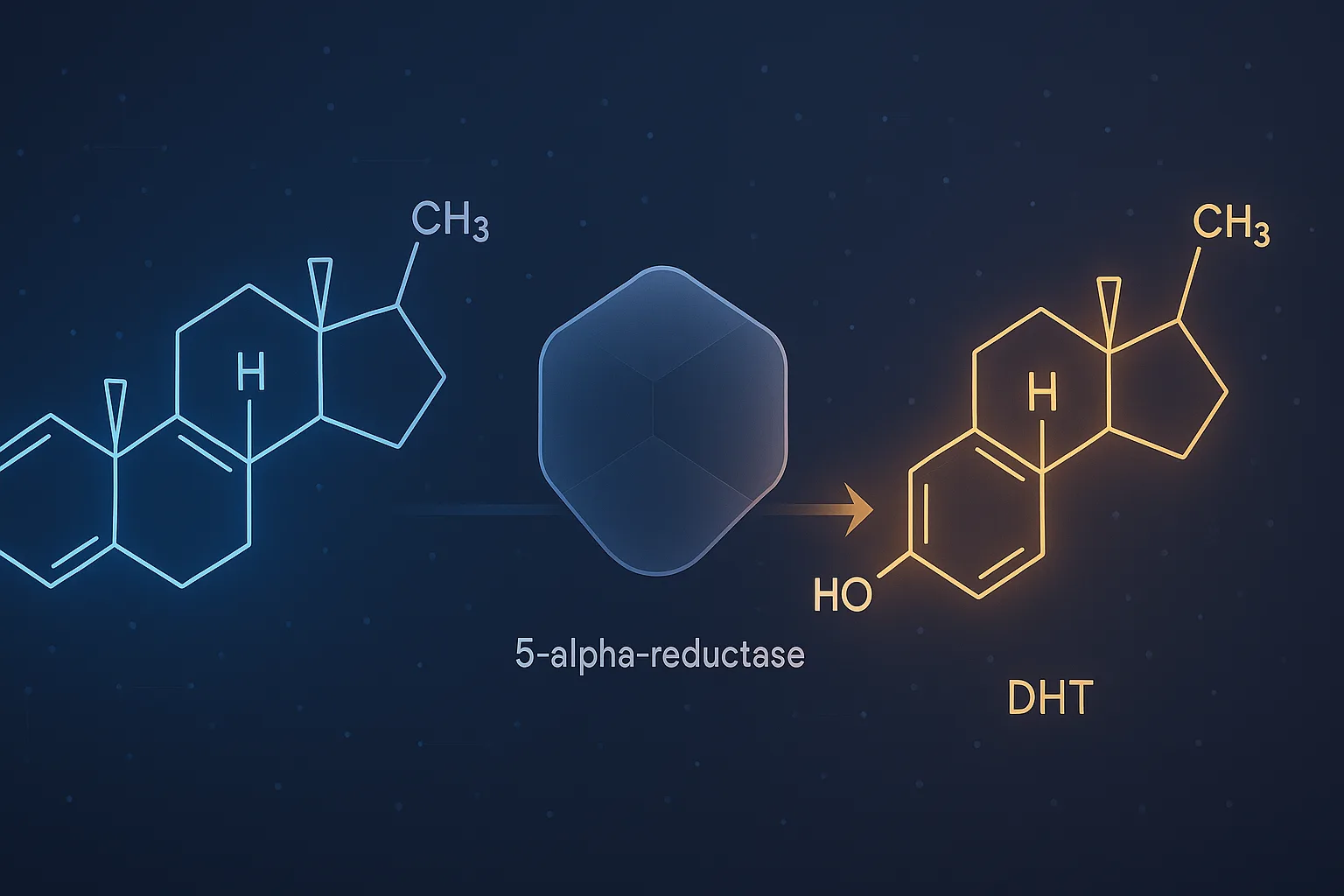
Dihydrotestosterone (DHT) is the most receptor-active androgen the human body produces. It is made by converting testosterone via an enzyme called 5-alpha-reductase, which is concentrated in skin, scalp follicles, the prostate, and the genitals. Once formed, DHT binds the androgen receptor with roughly 3-5x the affinity of testosterone and dissociates more slowly, which is why it produces strong tissue-level effects at relatively modest serum concentrations.
In adult men off therapy, DHT typically runs 30-85 ng/dL on a sensitive assay. It contributes to libido, erectile function, secondary sexual characteristics, beard and body hair growth, and male-pattern hair loss in genetically susceptible men. The same hormone drives both pubertal facial hair and pattern baldness -- the local tissue response determines which.
The math is simple: more substrate, more enzyme product. When TRT raises serum testosterone to the upper physiologic range (700-1100 ng/dL is typical at trough), 5-alpha-reductase has more testosterone to convert. The conversion rate is roughly stable per individual, so serum DHT rises proportionally.
Published pharmacokinetic data on intramuscular testosterone cypionate show DHT typically lifting from a baseline of 30-80 ng/dL to 70-180 ng/dL on standard dosing. Subcutaneous protocols sit close to intramuscular. Non-scrotal gels run somewhat higher because skin is rich in 5-alpha-reductase. Scrotal-application creams produce the highest DHT of any common preparation -- studies have documented DHT levels 3-5x above off-therapy baseline because scrotal skin has very high enzyme density.
The clinical question is not whether DHT rises -- it does -- but whether the rise matters for the individual man. For most men, it does not. DHT contributes to the libido benefit, the erectile improvement, and the secondary sexual characteristic effects that men actually report on TRT. Suppressing it without a reason removes some of that benefit.
When to Test DHT (and When to Skip It)
DHT does not belong on a routine TRT lab panel. The Endocrine Society 2018 guideline (Bhasin et al.) and the AUA 2018 guideline (Mulhall et al.) both list total testosterone, free testosterone or SHBG, estradiol, and CBC as the core monitoring set. DHT appears as a situational add-on, not a standing order.
Test DHT when a specific clinical question depends on the answer:
Order DHT when:
Hair loss is accelerating in the first 3-6 months and the question is whether to add a 5-alpha-reductase inhibitor
Acne is persistent past month 4 despite frequency adjustment and topical therapy, and DHT-blocker discussion is on the table
BPH symptoms (urinary urgency, slow stream, nocturia) are new or worsening
A man is on scrotal cream and the prescriber wants to confirm whether the high-DHT pattern matches the symptom complaint
The man is already on finasteride or dutasteride and the prescriber wants to confirm the drug is suppressing DHT as expected
Beard or body-hair growth pattern is changing in a way the patient finds clinically meaningful
Skip DHT when:
The man is asymptomatic, hematocrit is controlled, estradiol is in range, and total/free T are at goal
The reason for ordering is "curiosity" or "completeness" -- a number without a decision attached is noise
The man is in the first 6-8 weeks of any new protocol -- the lab is still moving, the decision will be premature
The clinic is charging for an expanded panel and the DHT result will not change the protocol
A useful framing: every lab on the panel should have a written if/then attached to it. If DHT is 80, do X. If DHT is 200, do Y. If you cannot write that sentence before you order the test, you do not need the test.
Lab reference ranges for DHT vary across methodologies. Liquid chromatography-mass spectrometry (LC-MS/MS) assays are the gold standard. Immunoassays still in use at some labs run higher and less reliably. When comparing DHT across draws, use the same lab and the same assay or the trend is unreliable.
Working interpretation framework on TRT:
DHT in the off-therapy reference range (typically 30-85 ng/dL): Unusual on TRT. Either the man is on a low replacement dose, has low 5-alpha-reductase activity, has been on a DHT-lowering agent, or the assay disagrees with the body of TRT literature. Recheck before acting.
DHT 70-180 ng/dL: Typical injectable-TRT pattern. If symptoms are absent, this is doing the work it is supposed to do.
DHT 180-300 ng/dL: Common on non-scrotal transdermal preparations or higher injectable doses. Investigate symptom side: acne, hair shedding, BPH, scalp itching, oily skin. If none, leave alone. If present, frequency-and-route adjustments come before drug intervention.
DHT above 300 ng/dL: Frequently seen on scrotal cream protocols. Route adjustment is usually the cleanest fix when symptoms are present.
The testosterone-to-DHT ratio is sometimes reported. In adult men off therapy the ratio typically runs 10:1 to 20:1 (T:DHT). On TRT the ratio narrows somewhat -- ratios of 7:1 to 12:1 are common and not abnormal. A very narrow ratio (under 5:1) suggests high 5-alpha-reductase activity, supraphysiologic DHT, or scrotal-cream delivery. A very wide ratio (over 25:1) suggests low 5-alpha-reductase activity, post-finasteride suppression, or recent dutasteride dose.
Symptoms That Track With High DHT
The decision to lower DHT should be driven by what the man is experiencing, not by the number in isolation. The androgenic-symptom cluster includes:
Hair shedding from genetically susceptible scalp regions (temples, crown, vertex). Hair shedding from the back of the head, eyebrows, or beard is not typically androgen-driven and points elsewhere. For the full evaluation, see TRT and hair loss prevention.
Acne on the back, shoulders, upper chest, and jawline -- the regions with high sebaceous-gland androgen receptor density. For the prevention and treatment ladder, see TRT acne management.
Persistent scalp itching, oily scalp, dandruff-like flaking that started after TRT began.
BPH-type urinary symptoms -- urgency, frequency, slow stream, nocturia, sense of incomplete emptying. PSA and an IPSS symptom score frame this evaluation.
Increased body hair growth in regions the patient finds clinically meaningful (back, shoulders). This is rarely a complaint that leads to DHT-lowering but is sometimes reported.
Notably absent from this list: libido, erectile function, muscle gain, mood, energy. These are mediated by testosterone and DHT together, and lowering DHT often subtracts from these benefits even when the man does not consciously notice it.
How to Lower DHT (In Order of Cost and Risk)
When DHT-related symptoms are clearly present and bothersome, the standard sequence is route first, frequency second, dose third, drug fourth. Jumping straight to finasteride or dutasteride skips three lower-risk interventions.
1. Change delivery route
The largest single-variable change in DHT comes from moving away from scrotal cream or non-scrotal transdermal toward injection. A man with DHT of 350 ng/dL on scrotal cream typically drops to 80-150 ng/dL on equivalent-dose intramuscular or subcutaneous injection within 6-8 weeks.
Weekly injections produce a peak-to-trough swing of roughly 2x in testosterone and a corresponding peak DHT spike. Splitting the same total weekly dose into twice-weekly or every-other-day injections flattens the curve and reduces the DHT peak without changing the total dose. Daily subcutaneous protocols produce the smoothest profile. See TRT injection frequency: weekly vs EOD.
3. Adjust total dose
A 20-30% dose reduction lowers DHT proportionally. The tradeoff is real -- it usually undoes some of the benefits that prompted starting TRT. This is a third-line intervention because the cost is symptomatic. See TRT dosing ranges and titrate TRT dose by trough levels for the dose-decision logic.
4. Topical anti-androgens
Topical saw palmetto, topical finasteride, topical ketoconazole shampoo, and topical minoxidil lower scalp DHT locally without meaningful systemic absorption. For a man whose only DHT-driven symptom is scalp hair shedding, this is often the cleanest intervention -- it targets the tissue where the symptom lives without changing systemic androgen exposure.
5. Oral finasteride or dutasteride
Systemic 5-alpha-reductase inhibition is the most effective DHT-lowering intervention and the one with the most baggage. Finasteride at 1 mg/day suppresses serum DHT by roughly 70%. Dutasteride at 0.5 mg/day suppresses serum DHT by 90%+ and has a much longer half-life.
The reasons to take these drugs seriously rather than reflexively:
Post-finasteride syndrome is real, if uncommon -- a minority of users report persistent sexual, neurological, or mood changes that persist after drug discontinuation. The exact incidence is debated, but the FDA labeling acknowledges the risk
Libido and erectile changes during use are reported in roughly 4-15% of users in the trial literature, higher in surveillance studies
Mood changes, including depression, are reported and are an FDA-labeled warning on finasteride
PSA suppression -- both drugs lower PSA by roughly 50%, which complicates prostate cancer screening. Prescribers typically double the measured PSA value to estimate the unadjusted reading
For most men with mild-to-moderate androgenic symptoms on TRT, the route-frequency-dose ladder resolves the issue without these drugs. For men with strong family history of pattern baldness who care about hair preservation and have tolerated the drugs in the past, the calculus is different.
What a Good Clinic Does With DHT
The clinic-evaluation angle on DHT is useful because it differentiates clinics quickly. A clinic that runs DHT on every patient at every visit is generating revenue, not information. A clinic that has never heard of DHT or refuses to order it when symptoms warrant is undertrained. The middle position -- order it situationally, interpret it with route and frequency context, use the route-frequency-dose ladder before drug intervention -- is what good prescribing looks like.
When evaluating a clinic, the relevant questions are:
Does the prescriber take an androgenic-symptom history at every follow-up (hair, acne, BPH symptoms, scalp), not just total T and energy?
If a patient develops hair shedding or persistent acne, does the clinic try frequency and route adjustments before reaching for finasteride?
Does the clinic offer a transdermal-to-injection switch as a route option, or are they locked into one delivery method for inventory reasons?
Does the prescriber explain the DHT result in context (route, frequency, symptoms) rather than treating the number as a verdict?
A clinic that dismisses androgenic symptoms, refuses to adjust the protocol, or jumps straight to 5-alpha-reductase inhibitors without route or frequency work is not running the protocol correctly. See TRT clinic red flags and questions to ask a TRT clinic for the broader evaluation framework. To compare clinics that handle protocol adjustments well, see the best online TRT clinic comparison.
The Anti-Overcorrection Rule
The reflex in TRT culture and on social media is to lower DHT prophylactically -- treat every man as if he is hair-loss prone, every dose as if it is causing acne, every prostate as if it is at risk. This is the same overcorrection pattern that drives blanket aromatase inhibitor prescribing in men who do not need it.
The data does not support this stance. The TRAVERSE trial and subsequent prostate-cancer meta-analyses found no increased prostate cancer risk at physiologic TRT doses. Most men do not develop bothersome acne, do not lose hair, do not develop BPH symptoms, and do not need DHT lowering. The men who do benefit are identifiable by symptoms and history -- not by a number on a lab.
The correct default is: leave DHT alone unless the patient is telling you it needs intervention. Test situationally. Adjust route and frequency before reaching for drugs. Document the symptom that justified the intervention so the prescribing record makes sense in twelve months.
When DHT Suggests Something Other Than TRT Response
Occasionally a DHT result points at a non-TRT issue and is worth investigating:
Very high DHT with a low testosterone-to-DHT ratio in a man who is not on scrotal cream -- check for adrenal androgen production, late-onset congenital adrenal hyperplasia (rare in adult presentation but exists), or supplement contamination
Very low DHT with normal total T and no finasteride/dutasteride use -- check for 5-alpha-reductase deficiency variants (rare) or assay issues
DHT response that does not match the route -- a man on injections with DHT in the 300 ng/dL range needs further evaluation, not a reflexive dose cut
These are uncommon and require endocrinology or specialty input. They are listed here because the routine TRT clinic will not always recognize them, and a knowledgeable patient can flag the pattern.
References
Bhasin S, Brito JP, Cunningham GR, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744.
Mulhall JP, Trost LW, Brannigan RE, et al. Evaluation and Management of Testosterone Deficiency: AUA Guideline. J Urol. 2018;200(2):423-432.
Lincoff AM, Bhasin S, Flevaris P, et al. Cardiovascular Safety of Testosterone-Replacement Therapy. N Engl J Med. 2023;389:107-117. (TRAVERSE trial — relevant to the DHT-prostate safety discussion.)
Marks LS, Mazer NA, Mostaghel E, et al. Effect of testosterone replacement therapy on prostate tissue in men with late-onset hypogonadism. JAMA. 2006;296(19):2351-2361.
Swerdloff RS, Wang C, White WB, et al. A New Oral Testosterone Undecanoate Formulation Restores Testosterone to Normal Concentrations in Hypogonadal Men. J Clin Endocrinol Metab. 2020;105(8):2515-2531. (DHT pharmacokinetics across formulations.)
McConnell JD, Wilson JD, George FW, et al. Finasteride, an inhibitor of 5 alpha-reductase, suppresses prostatic dihydrotestosterone in men with benign prostatic hyperplasia. J Clin Endocrinol Metab. 1992;74(3):505-508.
Andriole GL, Bostwick DG, Brawley OW, et al. Effect of dutasteride on the risk of prostate cancer (REDUCE trial). N Engl J Med. 2010;362(13):1192-1202.
No. DHT is a situational lab, not a routine one. Most prescribers do not check DHT at baseline or follow-up unless a man develops a specific androgenic symptom -- accelerated hair loss, persistent acne, prostate concerns, or scalp itching that started after TRT began. For an asymptomatic man with steady total T, free T, estradiol, and hematocrit, adding DHT to every panel produces a number with no decision attached to it.
What is a normal DHT level on TRT?
Reference ranges typically run 30-85 ng/dL in adult men off therapy. On TRT, DHT commonly rises into the 70-180 ng/dL range with intramuscular dosing and substantially higher with transdermal preparations, particularly scrotal cream. The absolute number matters less than the trajectory and whether symptoms are tracking with the rise. A DHT of 150 ng/dL in a symptom-free man on injections is not automatically a problem.
How does TRT delivery method change DHT?
Intramuscular and subcutaneous injections produce the lowest DHT relative to total testosterone. Non-scrotal transdermal gels and creams produce moderately higher DHT because skin is rich in 5-alpha-reductase. Scrotal-application creams produce the highest DHT of any common preparation, often 3-5x baseline, because scrotal skin has very high enzyme density. Pellets sit between injections and non-scrotal transdermals.
Will finasteride or dutasteride mess up my TRT results?
They do not lower testosterone meaningfully, but they alter the symptom picture. Finasteride blocks roughly 70% of scalp DHT conversion at 1 mg/day. Dutasteride blocks 90%+ of total-body DHT. Both can preserve hair and reduce androgenic acne. Both can also reduce libido, alter erectile function, and trigger mood changes in a minority of users. The tradeoff is real and personal -- it is not a free intervention.
Can I lower DHT without finasteride or dutasteride?
Yes, and the first move is usually changing delivery method, not adding a drug. Switching from a transdermal preparation to subcutaneous or intramuscular injections drops DHT substantially. Splitting weekly injections into more frequent smaller doses flattens the peak and reduces the peak DHT spike. Topical saw palmetto or topical anti-androgens reduce scalp DHT locally without systemic 5-alpha-reductase blockade. Dose reduction works but usually undoes the benefits that prompted starting therapy.
Does high DHT cause prostate problems?
The relationship is more complex than the legacy 'DHT drives prostate cancer' framing. The TRAVERSE trial and the prostate-cancer meta-analyses published since show no increased prostate cancer risk on TRT at physiologic doses. DHT can contribute to benign prostatic hyperplasia (BPH) symptoms -- urinary urgency, slow stream, nocturia -- and dutasteride is FDA-approved specifically for BPH. PSA, IPSS symptom score, and DRE are the standard monitoring tools, not DHT in isolation.