The injection method you choose for TRT affects more than just comfort. Subcutaneous and intramuscular injections differ in absorption rate, hormone stability, estradiol conversion, hematocrit impact, and long-term tissue effects. Most men default to intramuscular because that is what their clinic prescribed first. But the evidence increasingly favors subcutaneous for the majority of TRT patients.
Key Takeaways
Subcutaneous injections achieve the same therapeutic testosterone levels as intramuscular, with more stable day-to-day levels
SubQ produces lower estradiol and hematocrit spikes than IM due to slower, steadier absorption
SubQ uses smaller needles (27-31 gauge), is virtually painless, and eliminates the risk of hitting nerves or blood vessels in muscle
IM may still be preferred for high-volume injections (above 0.5 mL) or patients with very low body fat
Most modern TRT clinics now offer subcutaneous protocols, and many have made it their default
What Each Method Actually Means
Intramuscular (IM) Injection
Intramuscular injection delivers testosterone directly into skeletal muscle tissue. The oil-based testosterone sits in a depot within the muscle fibers, where it absorbs into the bloodstream through the muscle's dense capillary network.
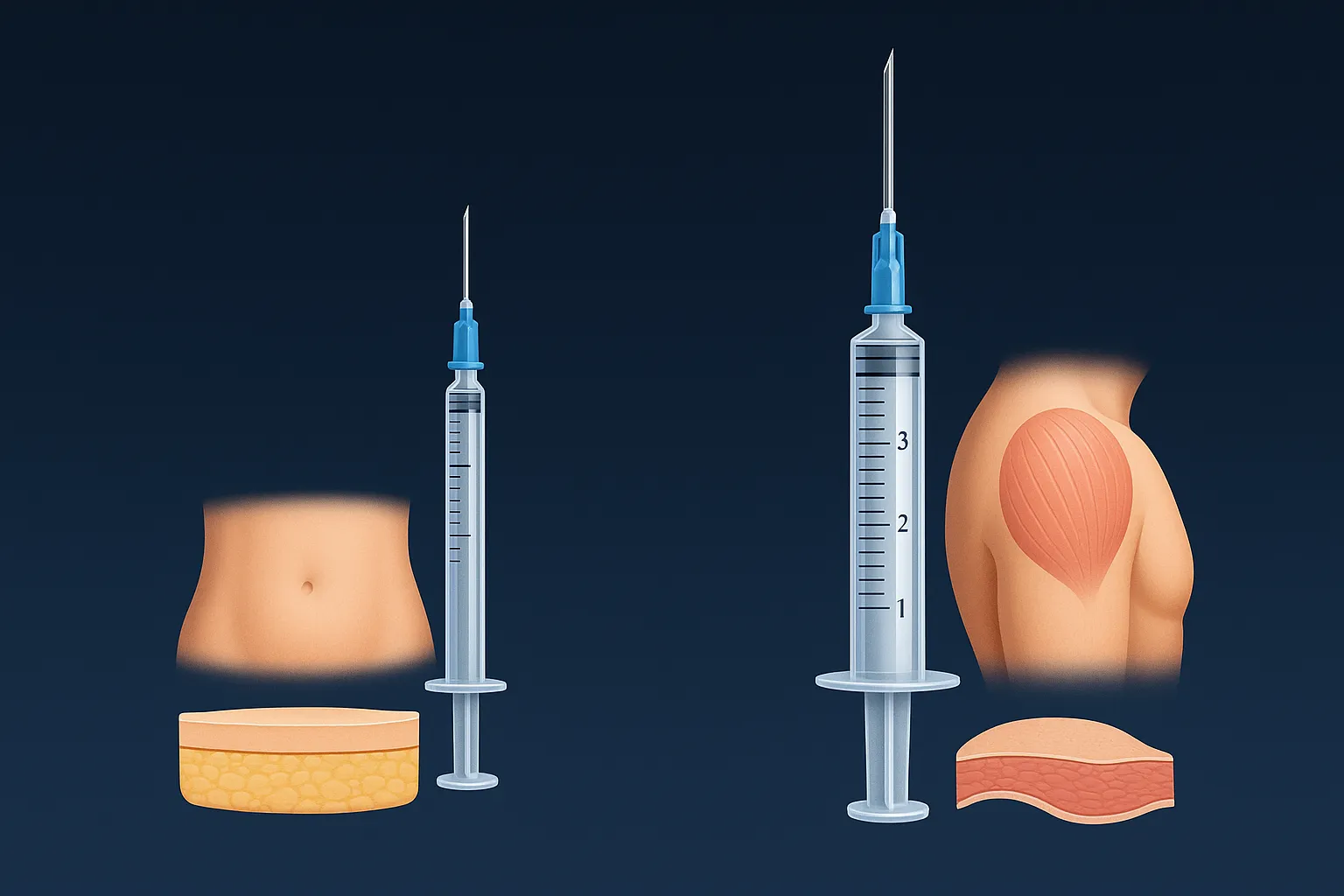
Common IM injection sites include the vastus lateralis (outer thigh), ventrogluteal (hip), and deltoid (shoulder). Needle length ranges from 1 to 1.5 inches with 23-25 gauge thickness, depending on the site and the patient's body composition.
IM injection has been the standard for testosterone replacement since the 1950s. It works. But "standard" does not mean "optimal."
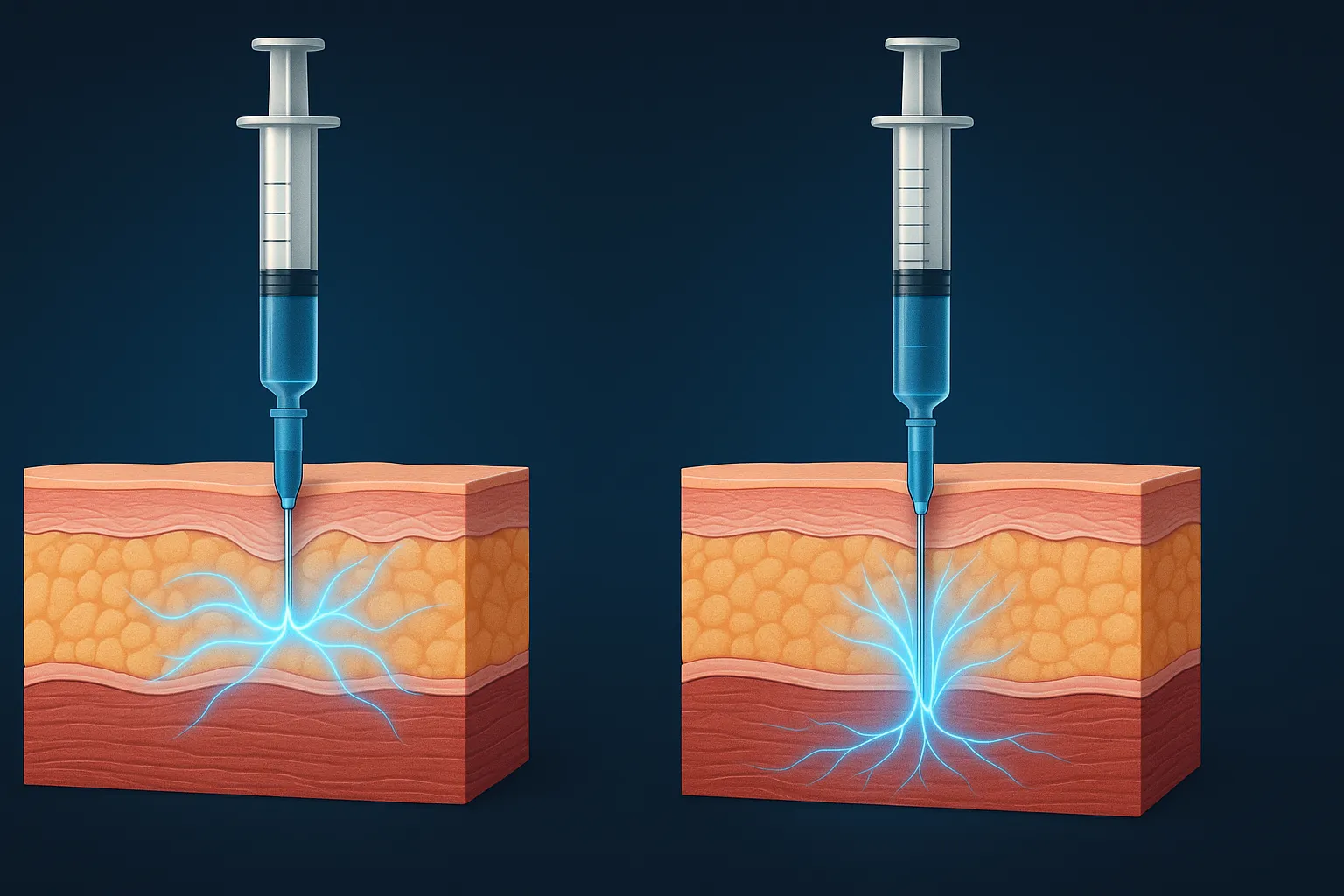
Subcutaneous (SubQ) Injection
Subcutaneous injection delivers testosterone into the fat layer just beneath the skin. The testosterone depot sits in adipose tissue, where it absorbs more slowly through the smaller capillary network in fat compared to muscle.
SubQ injection sites include the abdomen (at least 2 inches from the navel), the love handle area, the upper outer thigh, and the back of the arm. Needle length is typically 1/4 to 1/2 inch with 27-31 gauge thickness -- the same insulin syringes diabetics use millions of times daily.
SubQ testosterone gained clinical traction in the 2010s and is now widely adopted by progressive TRT clinics. The FDA-approved Xyosted autoinjector (subcutaneous testosterone enanthate) further legitimized the route.
See If You Qualify for Doctor-Supervised TRT
We'll match you with a licensed provider in your state — bloodwork, dosing, and ongoing telehealth follow-up.
Pharmacokinetics: How Absorption Differs
This is where the methods diverge meaningfully.
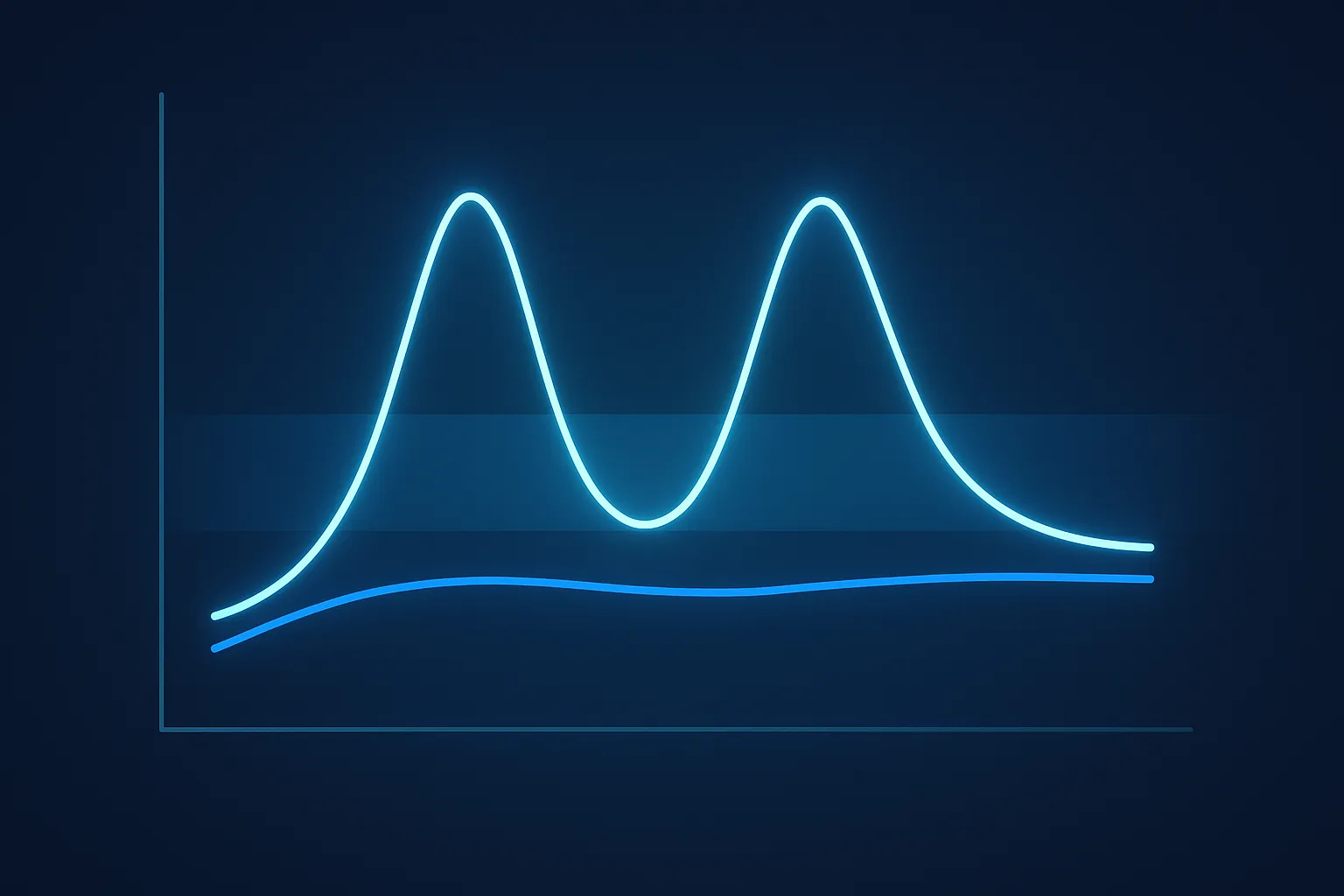
IM Absorption Pattern
Intramuscular injection creates a rapid absorption curve. Testosterone levels spike within 24-48 hours of injection, often reaching supraphysiological peaks (above 1,500 ng/dL on standard doses), then decline steadily until the next injection.
A study measuring hormone profiles after intramuscular testosterone enanthate found that serum estradiol levels increased 1.7-fold within 24 hours of injection, driven by the testosterone spike overwhelming the aromatase enzyme system [1]. This peak-and-crash pattern is what drives many of the side effects men associate with TRT -- mood swings, acne flares, and water retention that fluctuate with their injection schedule.
SubQ Absorption Pattern
Subcutaneous injection creates a flatter absorption curve. Adipose tissue has a less dense capillary network than muscle, so testosterone absorbs more gradually. The result is lower peaks and higher troughs -- a narrower band of testosterone fluctuation throughout the injection cycle.
A 52-week study of 150 hypogonadal men using weekly subcutaneous testosterone enanthate found that 92.7% achieved average total testosterone of 300-1,100 ng/dL (mean 553 ng/dL), with "small peak and trough fluctuations" [2]. The researchers specifically noted the pharmacokinetic profile was steady, a direct contrast to the rollercoaster pattern seen with IM.
A separate study in patients receiving weekly subcutaneous testosterone cypionate confirmed that total and free testosterone levels "remained stable between injections" throughout the dosing interval [3]. This stability is the core pharmacokinetic advantage of SubQ delivery.
Blood Level Stability
Stability matters because your body responds not just to average testosterone levels but to the rate of change. Rapid swings in testosterone trigger:
Estradiol spikes -- aromatase converts testosterone to estradiol proportionally to the peak, not the average
Hematocrit surges -- erythropoiesis responds to supraphysiological peaks
Mood instability -- neurosteroid levels fluctuate with testosterone
Energy crashes -- the trough before your next injection feels worse when the peak was higher
The flatter SubQ curve addresses all four of these. Men who switch from weekly IM to SubQ at the same dose frequently report feeling "more even" -- not higher or lower, but more consistent day to day.
Estradiol and Hematocrit: The Safety Argument
This is where the data gets compelling.
A comparative study of 234 hypogonadal men treated with either intramuscular testosterone cypionate or subcutaneous testosterone enanthate (both at 100 mg weekly) found significant differences in secondary markers [4]:
Estradiol: SubQ produced lower post-treatment estradiol levels than IM after adjusting for covariates
Hematocrit: SubQ was associated with lower post-therapy hematocrit elevations than IM
PSA: No significant difference between groups
The researchers concluded that subcutaneous testosterone enanthate "represents an effective testosterone delivery system with a potentially preferable safety profile over intramuscular testosterone cypionate."
This is not a minor distinction. Elevated hematocrit is the most common reason men are forced to reduce their TRT dose or donate blood. Elevated estradiol is the most common reason men are prescribed an aromatase inhibitor they may not need. If the injection route itself can reduce both of these problems without changing the dose, that is a meaningful clinical advantage.
The clinic landscape has shifted significantly in the past three years.
Clinics defaulting to SubQ: Most modern telehealth TRT clinics now start patients on subcutaneous protocols. The smaller needles, easier self-administration, and better side effect profile align with the telehealth model where patients manage their own injections at home. If you are evaluating online TRT clinics, ask specifically about their injection protocols.
Clinics still using IM: Traditional urology practices and some older clinics continue prescribing intramuscular injections, often biweekly at higher doses. This is partly institutional inertia -- IM has decades of clinical precedent -- and partly because some physicians are unfamiliar with the SubQ data.
Clinics offering both: The best clinics let patients choose after explaining both options, then adjust based on lab results and patient preference. A study of patients originally on IM who were offered the switch found that all 22 patients who tried SubQ expressed a preference for it -- none wanted to go back to IM [5].
Practical Injection Guidance
SubQ Technique
Equipment: 0.5 mL or 1 mL insulin syringe, 27-31 gauge, 1/2 inch needle. No separate drawing needle needed for small volumes -- insulin syringes can draw directly from the vial, though it takes 30-60 seconds for viscous testosterone oil through a fine gauge.
Site preparation: Clean the injection site with an alcohol swab. Let it air dry completely.
Injection steps:
Pinch a fold of skin and fat between your thumb and index finger at the injection site
Insert the needle at a 45-90 degree angle (45 degrees for lean individuals, 90 degrees if you have adequate subcutaneous fat)
Inject slowly -- 10-15 seconds for the full volume
Release the skin fold and withdraw the needle
Apply gentle pressure with a cotton ball if there is any bleeding
Volume limit: Keep individual SubQ injections to 0.5 mL or less per site. If your weekly dose requires more volume, split it across two sites or increase your injection frequency.
Site rotation: Rotate between at least 4-6 sites to prevent lipohypertrophy (hard lumps in the fat). The abdomen alone provides ample real estate -- think of it as a clock face around your navel, with injection sites at 2, 4, 8, and 10 o'clock positions, each at least 2 inches from the navel. For a full site rotation strategy, see our managing injection sites guide.
IM Technique
Equipment: 1 mL or 3 mL luer-lock syringe. Drawing needle: 18-21 gauge, 1 inch. Injection needle: 23-25 gauge, 1-1.5 inches.
Preferred sites:
Ventrogluteal (recommended): Place your palm on the greater trochanter, index finger on the anterior iliac crest, spread your middle finger toward the iliac crest -- inject in the V between your fingers. This site has the lowest nerve density and thickest muscle.
Vastus lateralis (outer thigh): The outer middle third of the thigh. Easy to self-inject but has more nerve endings.
Deltoid: Suitable for volumes under 1 mL. Convenient but limited by muscle size.
Injection steps:
Clean the site with an alcohol swab
Spread the skin taut with your non-dominant hand (Z-track technique: pull the skin to one side before inserting)
Insert the needle at 90 degrees in a smooth, dart-like motion
Aspirate briefly -- if blood appears, withdraw and try a different spot
SubQ wins for most TRT patients, but there are legitimate scenarios where intramuscular injection makes more sense:
High-volume doses. If your protocol requires more than 0.5 mL per injection and you inject once weekly, IM accommodates larger volumes more comfortably. Though the better solution is often splitting into smaller, more frequent SubQ doses.
Very low body fat. Men with extremely low subcutaneous fat (competitive bodybuilders in contest prep, for example) may not have adequate tissue depth for SubQ injection. If you can pinch less than 1/4 inch of skin and fat, SubQ becomes impractical.
Persistent SubQ nodules. A small percentage of patients develop firm, sometimes tender nodules at SubQ injection sites. If site rotation and volume reduction do not resolve this, switching to IM eliminates the issue.
Patient preference. Some men simply prefer IM after trying both. The data favors SubQ on average, but individual response varies. If your labs look good and you are comfortable with IM, there is no clinical reason to force a switch.
How to Switch from IM to SubQ
Switching is straightforward, but a few considerations matter:
Dose adjustment. Most clinics use the same dose when switching from IM to SubQ. However, because SubQ absorption is slower and steadier, some patients find they can achieve the same therapeutic levels at a slightly lower dose. Work with your clinic to check labs 6-8 weeks after switching.
Frequency. If you were injecting IM once weekly, you may benefit from splitting to twice weekly SubQ. The combination of SubQ's inherently steadier absorption plus increased frequency creates the flattest possible testosterone curve.
Expect a transition period. The first 2-3 weeks after switching may feel slightly different as your body adjusts to the new absorption pattern. Do not make dose changes based on how you feel during this transition -- wait for labs.
Keep your old supplies briefly. If you develop nodules or discomfort with SubQ, you can switch back to IM temporarily while troubleshooting site rotation and volume.
Standard TRT -- whether IM or SubQ -- is often prescribed at 100-200mg/week from day one -- doses calibrated to push levels well above mid-range fast. For some users, that jump is too much: energy spikes, mood swings, aggression, sleep disruption, or simply feeling "overly pumped up" in a way that doesn't match how they want to feel on TRT. SubQ's inherently flatter absorption curve smooths the peak, but the total weekly dose still determines where your average sits.
A conservative alternative starts at 25-50mg/week (~1/4 the standard starting dose) for 4-8 weeks, then titrates up only if blood work and symptoms warrant it. Because SubQ tops out at roughly 0.5mL per site, a smaller weekly dose fits neatly into a twice-weekly or daily insulin-syringe protocol. Reports from community and clinician notes increasingly favor this approach for users who are sensitive to hormonal changes or want a smoother adjustment curve. Some users find they never need the full dose -- they hit target free T levels and reach their goals at the lower end of the range.
This is not a universal recommendation. Some men genuinely need 150-200mg/week to achieve symptom relief, and aggressive titration is appropriate when labs show severe hypogonadism. But if you have room to negotiate dose with your prescriber, asking for a 4-8 week "start low, titrate slowly" phase is a legitimate choice that many users report worked better for them than jumping straight to a full replacement dose.
The Verdict
The evidence strongly favors subcutaneous injection for most TRT patients. SubQ delivers equivalent testosterone levels with better stability, lower estradiol conversion, lower hematocrit impact, less pain, easier self-administration, and no risk of hitting nerves or blood vessels.
The original pilot study on subcutaneous testosterone replacement, published in 2006, concluded that low-dose subcutaneous testosterone was a viable alternative to intramuscular injection for hypogonadal men [6]. Since then, every subsequent study has reinforced that finding, and the 2018 FDA approval of a subcutaneous testosterone product made it official.
If you are starting TRT, ask your clinic about subcutaneous protocols. If you are currently on IM and dealing with estradiol issues, hematocrit creep, injection anxiety, or energy crashes before your next shot, a switch to SubQ may resolve those problems without changing your dose.
The best injection method is the one that keeps your levels stable, your side effects minimal, and your adherence consistent. For most men, that is subcutaneous.
References
Fukami M, et al. Hormone profiles after intramuscular injection of testosterone enanthate in patients with hypogonadism. Endocrine Journal. 2006;53(3):305-310. PMID: 16710076
Kaminetsky J, et al. A 52-Week Study of Dose Adjusted Subcutaneous Testosterone Enanthate in Oil Self-Administered via Disposable Auto-Injector. Journal of Urology. 2019;201(3):587-594. PMID: 30296416
Olson J, et al. Serum Testosterone Concentrations Remain Stable Between Injections in Patients Receiving Subcutaneous Testosterone. Journal of the Endocrine Society. 2018;2(8):787-796. PMID: 29264562
Gittelman M, et al. Comparison of Outcomes for Hypogonadal Men Treated with Intramuscular Testosterone Cypionate versus Subcutaneous Testosterone Enanthate. Journal of Urology. 2022;207(3):677-683. PMID: 34694927
Spratt DI, et al. Subcutaneous Injection of Testosterone Is an Effective and Preferred Alternative to Intramuscular Injection: Demonstration in Female-to-Male Transgender Patients. Journal of Clinical Endocrinology & Metabolism. 2017;102(7):2349-2355. PMID: 28379417
Al-Futaisi AM, et al. Subcutaneous administration of testosterone. A pilot study report. Saudi Medical Journal. 2006;27(12):1843-1846. PMID: 17143361
McFarland J, et al. Testosterone Therapy With Subcutaneous Injections: A Safe, Practical, and Reasonable Option. Federal Practitioner. 2021;38(11):e8-e13. PMID: 34698352
Wilson DM, et al. Pharmacokinetics, safety, and patient acceptability of subcutaneous versus intramuscular testosterone injection for gender-affirming therapy: A pilot study. Transgender Health. 2018;3(1):174-180. PMID: 29367424
Is subcutaneous testosterone as effective as intramuscular?
Yes. Multiple studies show subcutaneous injections achieve therapeutic testosterone levels (300-1,100 ng/dL) comparable to intramuscular, with 92.7% of patients reaching target range in a 52-week trial.
Does subcutaneous testosterone cause less estrogen conversion?
Research shows subcutaneous injections produce lower estradiol levels than intramuscular injections, likely because the slower absorption avoids the supraphysiological testosterone spikes that drive aromatization.
Can I inject testosterone cypionate subcutaneously?
Yes. Testosterone cypionate and enanthate can both be injected subcutaneously. Many TRT clinics now prescribe subcutaneous protocols as their default, typically using insulin syringes with 27-31 gauge needles.
Which is more painful, SubQ or IM testosterone?
Most patients report subcutaneous injections as virtually painless compared to intramuscular. SubQ uses smaller needles (27-31 gauge vs 23-25 gauge) and shallower depth (1/4 to 1/2 inch vs 1 to 1.5 inches).