Good injection site management is what separates a comfortable, sustainable TRT experience from one plagued by lumps, pain, scar tissue, and dread. If you're going to inject testosterone multiple times per week for years, you need a system.
Why Rotation Matters
Every time a needle penetrates tissue, it causes microscopic trauma. Oil-based testosterone also creates localized inflammation as the body absorbs it. Inject into the same spot repeatedly, and that microscopic trauma accumulates into scar tissue -- dense, fibrous tissue that:
Makes future injections more painful (the needle has to push through harder tissue)
Reduces absorption (scar tissue has less blood flow than healthy muscle or fat)
Creates visible or palpable lumps
Can eventually make a site unusable
The solution is systematic rotation. Give each injection site enough rest between uses for tissue to fully recover before you return to it.
Building Your Rotation Schedule
For Twice-Weekly Injections (4 Sites Minimum)
If you inject Monday and Thursday, you need at least 4 sites so each site gets a full week of rest:
Week
Monday
Thursday
1
Right VG
Left VG
2
Right Delt
Left Delt
3
Right VG
Left VG
4
Right Delt
Left Delt
VG = Ventrogluteal. This simple 4-site rotation gives each spot 7 days to recover.
Better approach -- 6 sites:
Week
Monday
Thursday
1
Right VG
Left VG
2
Right Delt
Left Delt
3
Right Quad
Left Quad
4
Right VG
Left VG
Six sites mean each spot gets 10-14 days of rest. More sites = better long-term tissue health.
For EOD or Daily Injections (8+ Sites Recommended)
Daily injectors need the most sites. With 8 sites in rotation, each gets a full week of rest even with daily injections:
Right abdomen (SubQ)
Left abdomen (SubQ)
Right love handle (SubQ)
Left love handle (SubQ)
Right outer thigh (SubQ)
Left outer thigh (SubQ)
Right delt (shallow IM or SubQ)
Left delt (shallow IM or SubQ)
For daily SubQ injectors using insulin syringes with small volumes (0.1-0.15mL), each of these "sites" is actually a zone. You don't need to hit the exact same spot -- injecting within a 2-3 inch radius of the target area counts as the same general site but distributes the micro-trauma more broadly.
Tracking Your Rotation
Keep a simple log. Options that work:
Phone notes app: Date, site, any reactions
Calendar reminders: Set your injection schedule with the site listed in the event title
Injection tracking app: Several free apps designed for this exist on iOS and Android
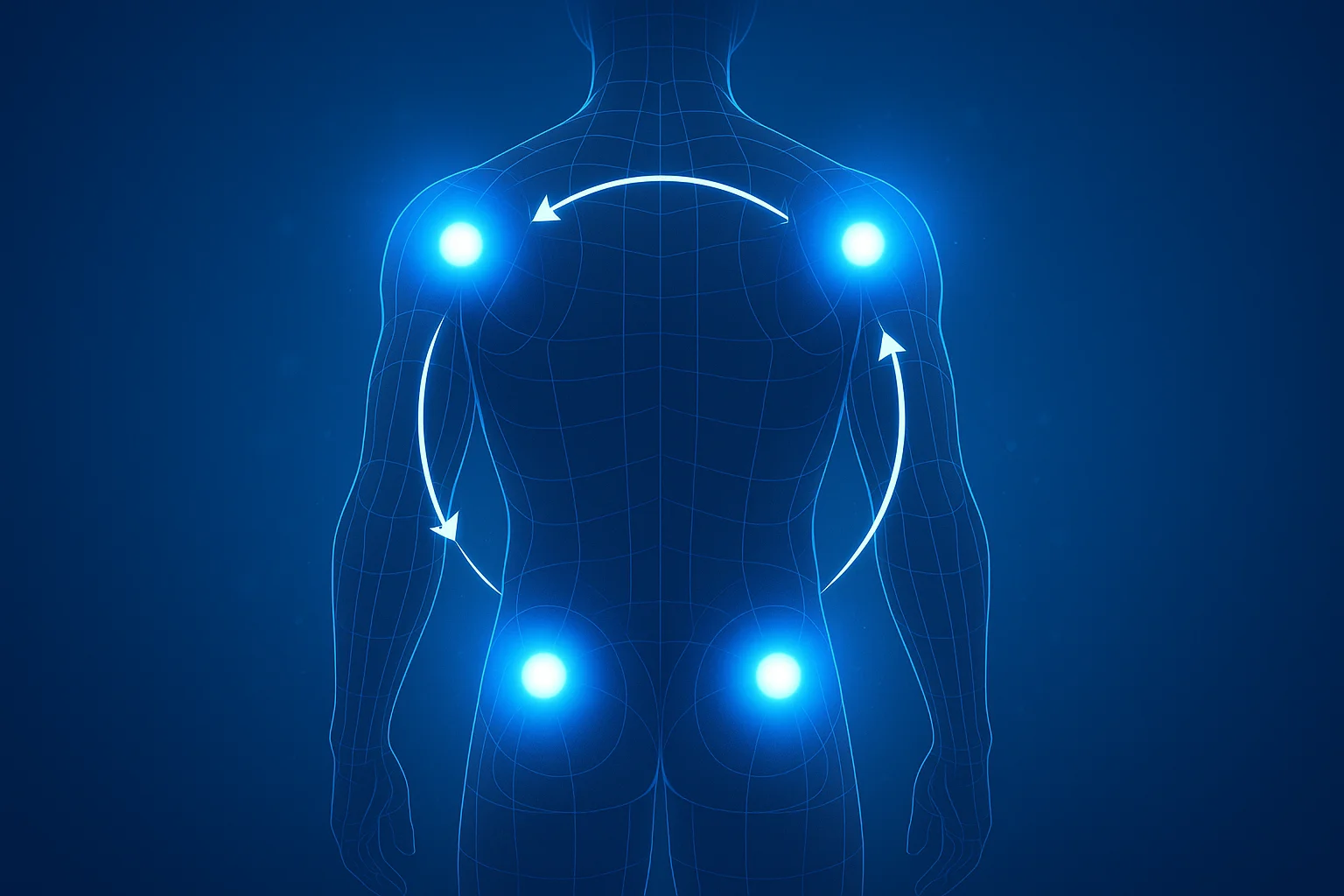
Simple rule: Move clockwise around your body. Right side, then left side. Top to bottom. Start over.
The method doesn't matter -- consistency does. Pick a system and stick with it. If you are new to injections, a good clinic will set up your rotation schedule during onboarding -- compare TRT clinics.
Why it's the best IM site: Thick muscle, minimal nerves and vessels, easy to access when you learn the landmark technique.
Tips:
Use your opposite hand to find the landmarks (palm on greater trochanter, index finger toward ASIS, middle finger toward iliac crest)
You can inject standing up or lying on your side with the top leg slightly forward
Insert the needle perpendicular to the skin surface, not angled toward your hip
This site tolerates larger volumes well (up to 2mL without discomfort for most men)
Common issue: Some men struggle to find this site at first. Have your provider mark it with a pen during a visit, or watch a reliable anatomical demonstration video.
Deltoid
Tips:
Keep volumes under 1mL
Use a 25-gauge, 1-inch needle for IM; 27-gauge, 0.5-inch for SubQ
Relax your arm completely -- don't flex the muscle. Let your arm hang at your side.
The injection site is 2-3 finger widths below the acromion (the bony point at the top of your shoulder)
Avoid injecting too low (toward the mid-arm) where the radial nerve runs
Common issue: Delts can be sore for 24-48 hours after injection, especially in the beginning. This is normal and doesn't indicate a problem.
Vastus Lateralis (Outer Quad)
Tips:
Sit with your leg relaxed, slightly bent
Target the middle third of the outer thigh
Insert at 90 degrees
This is one of the easiest sites for self-injection because you can see exactly what you're doing
Common issue: Quads are the most nerve-rich IM site used for TRT. Hitting a nerve causes a sharp, electric "zinger" that radiates down the leg. It's startling but harmless. If it happens, pull the needle out and shift your injection point slightly. Over time, you learn exactly where your nerves are and can avoid them.
Post-injection pain in the quads can be more pronounced than other sites. Some men love quad injections; others abandon them after a few attempts. Try it and see.
Abdomen (SubQ)
Tips:
Stay at least 2 inches from the navel
Avoid the midline -- inject to the left or right of center
Pinch a fold of skin and fat, inject at 45-90 degrees depending on body fat
Alternate between left and right sides, and vary the exact spot within each side
Keep volumes under 0.3-0.5mL per injection to avoid lumps
Common issue: Subcutaneous lumps. If you inject too much volume, the oil pools in the fat layer and forms a palpable lump that takes 3-7 days to absorb. Reducing volume per site or switching to more frequent smaller injections solves this.
Glute (Dorsogluteal)
Tips:
Always target the upper outer quadrant
Use a longer needle (1-1.5 inch) due to the fat layer over the glute
This site is harder to self-inject -- you need to twist your torso or use a mirror
Tolerates large volumes well (up to 3mL)
Common issue: Difficulty reaching the site consistently. If you can't see or comfortably reach your glute, use other sites instead.
Troubleshooting Injection Site Problems
Post-Injection Pain (PIP)
Mild soreness at the injection site for 24-72 hours is extremely common, especially with new sites, new esters, or higher-concentration testosterone.
Causes:
The oil itself causes localized inflammation (this is normal)
Benzyl alcohol and benzyl benzoate (preservatives in testosterone formulations) can irritate tissue
Injecting too quickly forces oil through tissue faster than it can accommodate
Cold oil is thicker and harder to disperse -- warming the vial to body temperature before injection helps
Injecting into a tense muscle increases trauma
Management:
Warm the vial by holding it in your hand or placing it in warm (not hot) water for a few minutes before drawing
Inject slowly -- take 20-30 seconds for the full volume
Relax the muscle completely before insertion
Apply gentle pressure after removing the needle
Light movement or walking after injection helps disperse the oil
Over-the-counter anti-inflammatory medication (ibuprofen) if needed
Lumps and Nodules
Subcutaneous lumps (SubQ injections): Usually caused by injecting too much volume into one spot. The oil pools and forms a firm, painless-to-mildly-tender lump that absorbs over 3-7 days. Reduce volume per site. If lumps are persistent, switch to IM.
Intramuscular nodules: A firm lump deep in the muscle that lasts more than a week may indicate the beginning of scar tissue formation. Increase your rotation to give that site more rest. If it persists for more than 2 weeks, have your provider evaluate it.
Bruising
Occasional bruising is normal -- you've nicked a small blood vessel. It's cosmetic and resolves on its own in 5-10 days.
To minimize bruising:
Apply firm pressure (don't rub) for 15-30 seconds after withdrawing the needle
Don't inject into areas where you can see veins through the skin
Avoid taking NSAIDs or fish oil immediately before injection, as they thin the blood
Oil Leaking (Depot Leakage)
Sometimes a small amount of oil leaks back out of the injection site after you withdraw the needle. This is common with IM injections and doesn't significantly affect your dose (the amount lost is minimal).
The Z-track method prevents this:
Before inserting the needle, use your non-dominant hand to pull the skin and subcutaneous tissue laterally (sideways) about 1 inch
Hold the skin displaced while you insert the needle and inject
After withdrawing the needle, release the skin
The skin moves back to its original position, creating a zigzag path that seals the injection tract
Redness, Warmth, and Swelling
Mild redness and warmth at the injection site for 24-48 hours can be a normal inflammatory response, especially with larger volumes or carrier oils your body is adjusting to.
Red flags that suggest infection:
Redness that spreads or worsens after 48 hours
Increasing pain, not decreasing
Warmth with fever or chills
Pus or discharge from the injection site
Red streaks extending from the site
If you see any of these signs, contact your provider. Injection site infections are rare with proper sterile technique but require prompt treatment with antibiotics if they occur.
Allergic Reactions to Carrier Oil
Testosterone is suspended in carrier oil -- commonly cottonseed oil (cypionate) or sesame oil (enanthate). Some men have allergies to these oils, which manifest as:
Persistent redness and itching at every injection site
Hives near the injection area
Excessive swelling beyond what's normal
If you suspect a carrier oil allergy, ask your provider to switch you to a different ester (which uses a different carrier oil) or request a compounded formulation in an alternative oil like grapeseed or MCT oil.
Long-Term Site Health
Annual Assessment
Once a year, do a self-assessment of your injection sites:
Are any sites consistently more painful than they used to be?
Can you feel hard, fibrous lumps in frequently used areas?
Has absorption from any site noticeably decreased (based on labs or symptoms)?
If a site is degrading, remove it from rotation for 2-3 months to allow recovery. Add a replacement site to maintain your rotation count.
Preventing Scar Tissue
The best prevention is consistent rotation. Beyond that:
Use the smallest effective needle gauge
Inject slowly and smoothly
Don't inject into a site that's still sore from the last injection
Vary your exact insertion point within each general site area
If a site consistently causes disproportionate pain, has developed palpable scar tissue, or shows signs of poor absorption, stop using it. The good news is that with proper rest (months to years), most scar tissue gradually remodels and the site can eventually return to rotation.
This content is for informational purposes only and is not medical advice. Consult a qualified healthcare provider before starting any treatment.
Frequently Asked Questions
How often should I rotate injection sites?
Rotate injection sites with each injection to prevent scar tissue buildup. Use at least 4-6 different sites in your rotation.
What do I do if I get lumps at injection sites?
Small lumps are normal but should resolve within a week. Persistent lumps may indicate scar tissue formation or infection requiring medical evaluation.