Perimenopause Gut Health: Why Digestion Changes and How HRT Helps
5/22/2026
5 min read
By The TRT Catalog
94% of menopausal women report digestive symptoms. Here's how estrogen decline disrupts your gut, what the estrobolome is, and which HRT protocols restore normal digestion.
Key Takeaways: 94% of perimenopausal and menopausal women report digestive symptoms, and 82% say those symptoms started or worsened during the menopause transition. The mechanism is hormonal: estrogen and progesterone regulate gut motility, the gut-brain axis, microbial diversity, and bile acid metabolism. The estrobolome -- gut bacteria that recycle estrogen via beta-glucuronidase -- loses capacity as microbial diversity drops, creating a feedback loop where declining hormones damage the gut and a damaged gut accelerates hormonal decline. HRT stabilizes the hormonal substrate and can improve digestive symptoms as a secondary benefit. Transdermal estradiol is preferred over oral for GI-symptomatic women because it avoids first-pass liver effects. A layered approach -- HRT plus targeted probiotics, dietary fiber, and stress management -- produces better outcomes than any single intervention.
The Digestive Symptoms No One Warned You About
The pattern is remarkably consistent. A woman in her early to mid 40s starts noticing bloating that will not resolve, constipation that alternates with loose stools, acid reflux after meals that never caused problems before, and a vague abdominal discomfort that diet changes, elimination protocols, and over-the-counter antacids barely touch.
She sees her primary care doctor. Maybe a gastroenterologist. She gets an IBS diagnosis, a prescription for a proton pump inhibitor, and advice to eat more fiber. The symptoms persist because no one connects them to the hormonal transition happening at the same time.
This is not a rare scenario. A 2025 study presented at the Menopause Society annual meeting in Orlando surveyed nearly 600 women aged 44 to 73 and found that 94% reported digestive health symptoms [1]. The most common: bloating (77%), constipation (54%), stomach pain (50%), and acid reflux (49%). Most critically, 82% reported that their digestive symptoms either started or worsened during perimenopause or menopause. Only 33% had received a formal IBS diagnosis despite the high symptom burden, and among the 53% who sought professional help, 58% considered the care inadequate.
These are not niche complaints. Digestive disruption is one of the most common yet least discussed symptoms of the menopause transition.
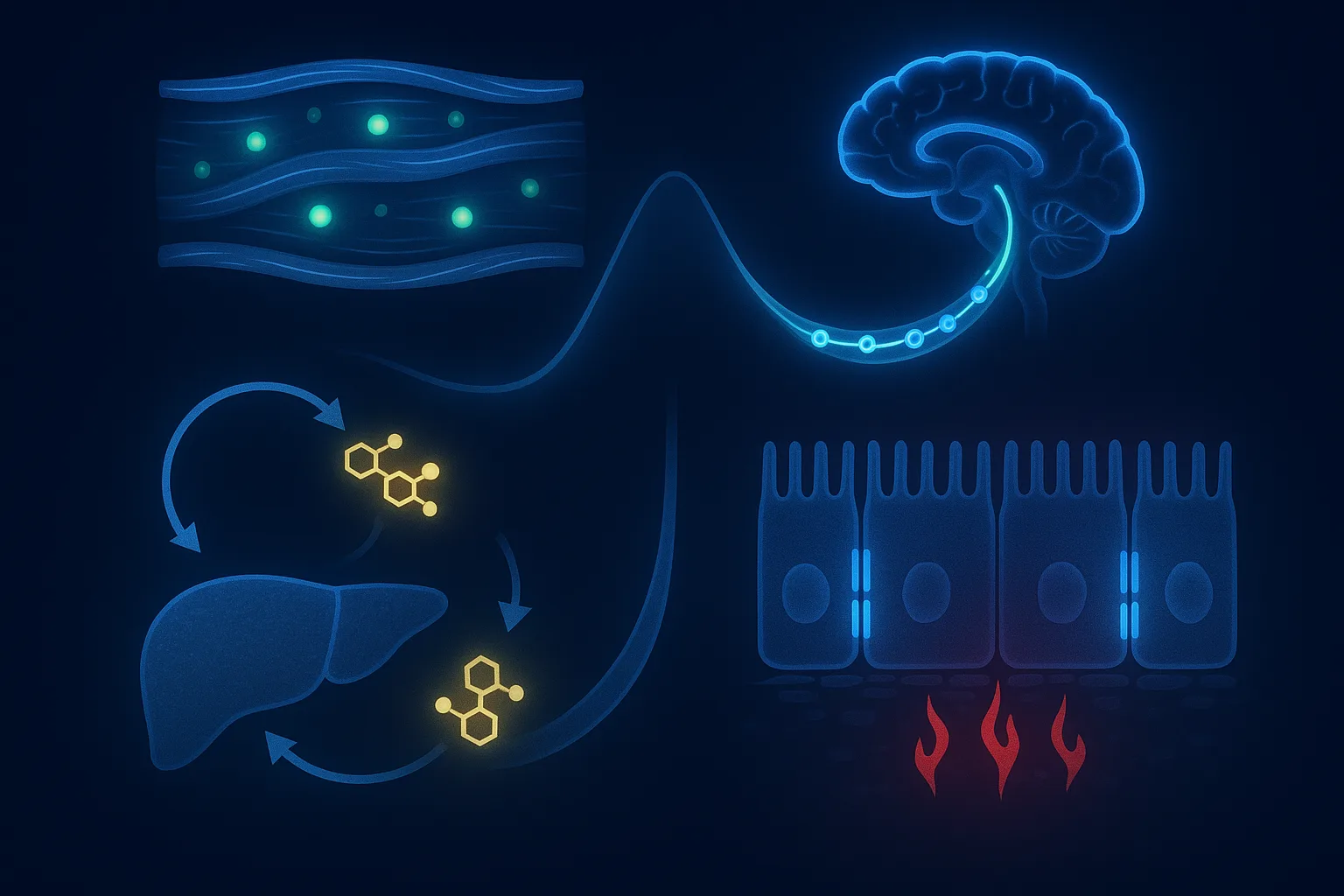
How Estrogen and Progesterone Regulate Your Gut
Your gastrointestinal tract is dense with estrogen and progesterone receptors. These hormones do not just affect your reproductive system -- they regulate multiple aspects of digestive function.
Gut Motility
Estrogen influences the speed at which food moves through the digestive tract. Estrogen receptors (ER-alpha and ER-beta) are present throughout the smooth muscle of the intestinal wall, where they modulate contraction patterns. Progesterone has a direct relaxing effect on smooth muscle, which is why constipation and bloating are common in the luteal phase of the menstrual cycle and during pregnancy when progesterone is high.
During perimenopause, the problem is not simply low hormones -- it is volatile hormones. Anovulatory cycles produce unpredictable progesterone drops and estradiol surges, which means gut motility oscillates between sluggish (high progesterone phases) and unstable (sudden hormone withdrawal). The net effect for most women is slower transit overall, leading to constipation, gas retention, and the characteristic bloating.
The Gut-Brain Axis
The enteric nervous system -- sometimes called the "second brain" -- contains over 100 million neurons and communicates bidirectionally with the central nervous system via the vagus nerve. Estrogen modulates both serotonin synthesis and serotonin receptor density, and approximately 90% of the body's serotonin is produced in the gut.
When estradiol fluctuates during perimenopause, serotonin signaling in the gut becomes erratic. This disrupts the coordinated contractions (peristalsis) that move food through the intestine and increases visceral hypersensitivity -- the heightened perception of normal digestive sensations as painful. This is the same mechanism that drives IBS, which is why IBS symptoms and perimenopausal digestive complaints overlap so heavily.
Bile Acid Metabolism
Estrogen regulates bile acid synthesis and the enterohepatic circulation of bile salts. During menopause, altered bile acid metabolism can change stool consistency, increase acid reflux, and contribute to the nausea and upper GI discomfort that some women report. This is a less discussed mechanism but explains why acid reflux -- a top-four symptom in the Menopause Society survey -- appears or worsens during the transition.
Intestinal Barrier Function
Estrogen helps maintain the integrity of the intestinal epithelial barrier -- the single-cell-thick lining that separates the gut contents from the bloodstream. When estrogen declines, barrier permeability may increase, allowing bacterial endotoxins (lipopolysaccharides) to cross into the bloodstream and trigger low-grade systemic inflammation. This "leaky gut" mechanism is implicated in the widespread inflammatory symptoms many women experience during menopause, from joint pain to brain fog to skin changes.
The Estrobolome: Your Gut Bacteria Regulate Your Hormones
One of the most important concepts in understanding the gut-hormone connection is the estrobolome -- the collection of bacterial genes in the gut microbiome that encode enzymes capable of metabolizing estrogen [2].
How It Works
The liver metabolizes circulating estrogen and packages it as conjugated (inactive) estrogen, which is excreted into the intestine via bile. In a healthy gut, estrobolome bacteria produce an enzyme called beta-glucuronidase, which converts this conjugated estrogen back to its active, unconjugated form. The reactivated estrogen is then reabsorbed through the intestinal wall and re-enters circulation. This is the enterohepatic recycling of estrogen -- and the gut microbiome is the gatekeeper.
What Happens During Menopause
Research published in Frontiers in Endocrinology in 2025 documented the microbial shifts that occur [2]:
Lactobacillus and Bifidobacteria -- key beneficial species -- markedly decline
Firmicutes and Roseburia species are depleted
Bacteroidetes and Enterobacter (potentially harmful species) increase
Overall microbial diversity drops significantly
A 2022 study in mSystems examining the Hispanic Community Health Study/Study of Latinos found that postmenopausal women had significantly lower abundance of the beta-glucuronidase gene compared to premenopausal women, and that several menopause-depleted bacterial species correlated directly with this gene [3]. The clinical implication: less beta-glucuronidase means less estrogen recycling, which means even lower effective estrogen levels than ovarian decline alone would produce.
The Feedback Loop
This creates a vicious cycle:
Ovarian estrogen production declines during perimenopause
Lower estrogen reduces gut microbial diversity, including estrobolome bacteria
Reduced estrobolome activity decreases estrogen recycling, further lowering circulating estrogen
Lower estrogen further impairs gut function -- motility slows, barrier integrity weakens, inflammation rises
The cycle accelerates
This feedback loop explains why some women experience a rapid cascade of worsening symptoms -- digestive, hormonal, inflammatory, and metabolic -- that seems disproportionate to the gradual decline in ovarian function. The gut is amplifying the hormonal signal.
Women's HRT — Menopause-First Telehealth
Bioidentical estradiol, progesterone, and low-dose testosterone — all 50 states, unlimited physician access.
The direct randomized evidence on HRT for digestive symptoms specifically is limited. But the mechanistic case is strong, and clinical observations are consistent.
What the Evidence Supports
By stabilizing estrogen levels, HRT can:
Restore estrogen receptor signaling in the gut wall, supporting normal motility patterns
Provide the hormonal substrate that gut bacteria need to maintain diversity and estrobolome function
Stabilize serotonin signaling in the enteric nervous system, reducing visceral hypersensitivity
Support intestinal barrier integrity, reducing endotoxin translocation and systemic inflammation
Women who start transdermal estradiol for vasomotor symptoms (hot flashes, night sweats) frequently report improvement in bloating, constipation, and IBS-like complaints as a secondary benefit. This is not placebo -- it follows directly from the hormonal mechanisms driving the digestive symptoms.
Why Transdermal Over Oral
For women with GI symptoms, the route of estrogen delivery matters:
Oral estrogen is absorbed from the gut and passes through the liver before entering general circulation (first-pass metabolism). This first-pass effect increases production of clotting factors, SHBG, inflammatory markers, and bile acid changes that can worsen nausea, reflux, and GI discomfort -- particularly in the first weeks of treatment.
Transdermal estradiol (patch, gel, or spray) is absorbed through the skin directly into systemic circulation, bypassing the liver entirely. This avoids the first-pass GI and hepatic effects, produces steadier blood levels, and is better tolerated by women whose digestive system is already symptomatic.
For women whose primary complaint is digestive, transdermal delivery is the clear first choice. See the estradiol patch dosing guide for practical dosing details.
Progesterone Considerations
Oral micronized progesterone (100-200 mg at bedtime) is required for endometrial protection in women with an intact uterus taking systemic estrogen. It has a mild sedating effect via GABA-A receptor modulation that often improves sleep.
However, progesterone's smooth-muscle relaxing properties can worsen constipation and bloating in some women, particularly in the first 4-6 weeks. If GI symptoms worsen on oral progesterone, options include:
Reducing the dose (100 mg rather than 200 mg if clinically appropriate)
Switching to a progestogen-releasing IUD (Mirena) for local endometrial protection without systemic GI effects
Cyclical rather than continuous progesterone (14 days per month rather than daily)
The Practical 2026 Protocol for Gut Health in Perimenopause
Managing perimenopause-related digestive symptoms works best as a layered approach that addresses the hormonal driver and the microbiome simultaneously.
Layer 1: Address the Hormonal Substrate
If you have perimenopausal symptoms beyond just GI complaints (hot flashes, sleep disruption, mood changes, cycle irregularity), HRT addresses the root hormonal driver:
Transdermal estradiol (0.025-0.1 mg/day patch, or equivalent gel/spray) -- stabilizes estrogen, avoids GI first-pass effects
Micronized progesterone at bedtime if uterus is intact -- monitor for constipation worsening; switch to IUD delivery if problematic
Optional low-dose transdermal testosterone if fatigue, low libido, and muscle loss accompany the digestive symptoms
A comprehensive hormone evaluation (FSH, estradiol, progesterone, free and total testosterone, SHBG) establishes where you are in the transition and guides treatment. See the best online HRT clinics for women for providers who evaluate the full hormonal picture alongside symptom assessment.
Layer 2: Support the Microbiome
While HRT addresses the hormonal substrate, targeted microbiome support helps restore the estrobolome and overall gut function:
Probiotics with clinical evidence in menopause:
Lactobacillus rhamnosus, L. reuteri, L. casei, L. helveticus -- species shown to improve microbial diversity and metabolic markers in menopausal women [2]
Bifidobacterium longum -- demonstrated benefits for emotional regulation and lipid metabolism during menopause
Look for multi-strain formulations with at least 10 billion CFU; take consistently for 8-12 weeks before assessing response
Prebiotic fiber:
25-30 grams of fiber daily from diverse plant sources -- vegetables, legumes, whole grains, nuts, seeds
Specific prebiotics: inulin, fructo-oligosaccharides (FOS), galacto-oligosaccharides (GOS) feed beneficial bacteria including estrobolome species
Increase gradually -- jumping from 10 to 30 grams of fiber overnight will worsen bloating before it improves
Fermented foods:
Yogurt, kefir, sauerkraut, kimchi, miso -- provide live cultures and the substrates they thrive on
A 2021 Stanford study found that a high-fermented-food diet increased microbial diversity and decreased inflammatory markers more effectively than a high-fiber diet alone
Layer 3: Dietary Modifications That Actually Help
Beyond fiber, several dietary strategies address the specific mechanisms of perimenopausal GI disruption:
Phytoestrogens: Soy isoflavones, flaxseed lignans, and other plant estrogens are converted by gut bacteria into bioactive metabolites (equol, enterolactone) with mild estrogenic activity [2]. These compounds support estrogen receptor signaling in women whose own production is declining. Not a replacement for HRT, but a meaningful dietary layer.
Anti-inflammatory foods: Omega-3 fatty acids (fatty fish, walnuts, flaxseed), polyphenols (berries, green tea, dark chocolate), and turmeric/curcumin reduce the gut inflammation that accompanies microbial disruption.
Reduce known triggers: Alcohol, caffeine, carbonated drinks, and highly processed foods each independently worsen gut motility, barrier function, and microbial diversity. During the perimenopausal transition, the gut is less resilient to these inputs.
Meal timing and portion size: Smaller, more frequent meals reduce the motility burden on a sluggish gut. Eating the largest meal at midday rather than evening aligns with the circadian rhythm of digestive enzyme production.
Layer 4: Stress and Nervous System Regulation
The gut-brain axis means that stress management is not a soft add-on -- it is a core component of GI treatment.
Vagal tone exercises: Slow diaphragmatic breathing (4-7-8 pattern), cold water face immersion, and humming/gargling stimulate the vagus nerve and improve gut-brain communication
Regular exercise: 150 minutes per week of moderate activity plus 2-3 sessions of resistance training improves gut motility, microbial diversity, and stress resilience simultaneously
Sleep optimization: Sleep deprivation independently disrupts the microbiome; micronized progesterone at bedtime serves double duty here
Mindfulness-based stress reduction (MBSR): Specifically studied for IBS, with demonstrated improvement in symptom severity, visceral sensitivity, and quality of life
When to Get a Full Workup
Digestive symptoms that appear or worsen in your late 30s to 50s deserve a dual evaluation -- GI and hormonal:
GI workup (rule out structural causes):
Celiac panel if not previously tested
H. pylori testing if upper GI symptoms predominate
Colonoscopy if age-appropriate or if symptoms include alarm features (blood in stool, unintentional weight loss, family history of colorectal cancer)
Thyroid function (TSH, free T4) -- hypothyroidism causes constipation and bloating and often co-occurs with perimenopause
Hormonal evaluation:
FSH, estradiol (day 2-3 if still cycling)
Progesterone (day 21 if still cycling, to confirm ovulation status)
Free and total testosterone, SHBG
DHEA-S
Comprehensive metabolic panel
The critical step is connecting the GI findings to the hormonal picture. A normal colonoscopy plus elevated FSH and erratic estradiol in a 44-year-old with new bloating and constipation is not "IBS" -- it is perimenopausal gut disruption, and the treatment approach is different.
What the Research Is Still Figuring Out
The gut-hormone field is moving fast, but important questions remain.
A 2026 systematic review and meta-analysis by Saravinovska et al. published in Frontiers in Endocrinology examined gut microbiome composition between women with low estrogen (postmenopausal and premature ovarian insufficiency) and euestrogenic controls. The analysis found no significant differences in alpha-diversity or Bacteroidetes-to-Firmicutes ratio between groups [4]. The authors attributed this to substantial heterogeneity across studies, limited control of confounding factors, and methodological variability.
This does not invalidate the estrobolome concept -- it highlights that the relationship between estrogen and the microbiome is more nuanced than "low estrogen equals low diversity." Individual variation in diet, geography, medication use, and baseline microbiome composition likely modulates the response. The 2025 Wang et al. review [2] and the 2022 mSystems study [3] found significant associations using different methodologies and populations.
What this means practically: the science supports addressing both the hormonal substrate and the microbiome, but the optimal probiotic strains, dosing, and combination with HRT have not been established in large randomized trials. The layered approach outlined above is based on the best available evidence, mechanism, and clinical observation -- which is where most of women's health treatment protocols stand in 2026.
What This Means for You
If your digestion changed during perimenopause, you are in the overwhelming majority -- not a minority with a mysterious condition. The mechanism is clear: hormones regulate your gut at every level, from motility to microbial composition to barrier integrity to the brain-gut signaling that coordinates it all.
The practical path forward:
Connect the dots -- if GI symptoms appeared alongside other perimenopausal symptoms, they are likely hormonally driven
Get a hormonal evaluation alongside any GI workup, not instead of one
Consider transdermal HRT as a first-line intervention that addresses the root hormonal driver
Layer in microbiome support -- probiotics, prebiotic fiber, fermented foods, phytoestrogens
Manage stress and sleep as core GI treatments, not optional add-ons
Give it time -- gut remodeling takes 8-12 weeks of consistent intervention
For women navigating new digestive symptoms in midlife, comprehensive women's hormone clinics evaluate the full hormonal, metabolic, and digestive picture together rather than treating each system in isolation. See the best online HRT clinics for women comparison for providers who take this integrated approach.
Denby N, et al. Menopause and the Gut: Uncovering a Hidden Health Burden. Poster presented at: Annual Meeting of The Menopause Society; October 21-25, 2025; Orlando, FL.
Wang H, Shi F, Zheng L, et al. Gut microbiota has the potential to improve health of menopausal women by regulating estrogen. Front Endocrinol. 2025;16:1562332. doi:10.3389/fendo.2025.1562332
Peters BA, Lin J, Qi Q, et al. Menopause Is Associated with an Altered Gut Microbiome and Estrobolome, with Implications for Adverse Cardiometabolic Risk in the Hispanic Community Health Study/Study of Latinos. mSystems. 2022;7(3):e00273-22. doi:10.1128/msystems.00273-22
Saravinovska A, et al. The impact of estrogen status on the gut microbiome: a systematic review and meta-analysis. Front Endocrinol. 2026;17:1780806. doi:10.3389/fendo.2026.1780806
Frequently Asked Questions
Why does perimenopause cause bloating and digestive problems?
Estrogen and progesterone both regulate gut motility, the gut-brain axis, and the composition of the gut microbiome. During perimenopause, erratic hormone fluctuations slow intestinal transit, alter bile acid metabolism, increase visceral sensitivity, and reduce the diversity of beneficial gut bacteria -- particularly the estrobolome, a collection of bacteria that metabolize estrogen. The result is bloating, constipation, acid reflux, and stomach pain that 94% of perimenopausal and menopausal women report in surveys. These symptoms are not psychological and not coincidental -- they have a clear hormonal mechanism.
What is the estrobolome and why does it matter in menopause?
The estrobolome is the subset of gut bacteria that produce beta-glucuronidase, an enzyme that converts conjugated (inactive) estrogen back to its active form for reabsorption through the intestinal wall. In premenopause, a healthy estrobolome maintains estrogen recycling. When menopause reduces estrogen levels and microbial diversity drops in parallel, the estrobolome loses capacity. Less estrogen is recirculated, which further reduces estrogen levels -- creating a feedback loop. This is why gut health and hormone health are bidirectional: a disrupted gut worsens hormonal symptoms, and hormonal decline disrupts the gut.
Does HRT help with perimenopause digestive issues?
Evidence is indirect but supportive. By stabilizing estrogen levels, HRT can restore estrogen receptor signaling in the gut wall, support normal motility, and provide the hormonal substrate that gut bacteria need to maintain diversity. Women who start transdermal estradiol for vasomotor symptoms frequently report improvement in bloating, constipation, and IBS-like complaints as a secondary benefit. However, oral estrogen may initially worsen some GI symptoms due to first-pass hepatic effects. Transdermal delivery avoids this.
Can probiotics replace HRT for menopause gut issues?
No. Probiotics and HRT address different layers of the problem. A 2025 randomized controlled trial showed that a probiotic formula with beta-glucuronidase activity regulated serum estrogen levels in postmenopausal women compared to placebo. But probiotics cannot replace the systemic estrogen that HRT provides. The most effective approach is layered: HRT to restore the hormonal substrate, plus targeted probiotics and dietary fiber to support the microbiome that metabolizes it.
Is menopause bloating different from regular bloating?
Yes. Menopause-related bloating has a hormonal driver that distinguishes it from dietary or functional bloating. It often worsens cyclically in perimenopause (tracking with anovulatory surges), persists despite dietary changes that would resolve ordinary bloating, and co-occurs with other perimenopausal symptoms like hot flashes, sleep disruption, and mood changes. Women describe it as a constant low-grade abdominal distension that diet alone cannot fix -- because the root cause is hormonal, not dietary.
Should I see a gastroenterologist or a hormone specialist?
Start with a clinician who understands hormonal contributions to GI symptoms. Many women see a gastroenterologist first, receive an IBS diagnosis, and get standard GI treatment that helps marginally because the hormonal driver is never addressed. If your digestive symptoms appeared or worsened in your late 30s to 50s alongside other perimenopausal symptoms, a hormone evaluation (FSH, estradiol, progesterone) alongside a GI workup provides the full picture. See our comparison of women's hormone clinics for providers who evaluate the complete hormonal picture.