
Key Takeaways: Perimenopausal estrogen fluctuations are a potent migraine trigger -- about two-thirds of women with prior hormonal migraine see worsening during the menopausal transition. The treatment lever is stability, not avoidance: transdermal estradiol at the lowest effective dose plus continuous (not cyclic) progesterone produces steadier hormone levels and lower attack frequency than oral or cyclic regimens. Migraine with aura is a contraindication to combined oral contraceptives but is not a contraindication to body-identical transdermal HRT, because physiologic estradiol does not carry the same thrombotic risk as ethinylestradiol. Most responders see improvement within 2 to 3 months of stable dosing.
The Problem No Headache Specialist Owns
A woman in her late 40s who has had occasional menstrual migraines for 20 years suddenly finds her cycle going haywire and her migraines exploding -- four to ten per month, sometimes with aura, sometimes wiping out entire weekends. Her primary care provider tells her it is stress. Her gynecologist tells her to wait it out. Her neurologist offers a triptan and increases her preventive medication. Nobody mentions that her estrogen is on a roller coaster and that the roller coaster is the problem.
Migraine and the menopausal transition are tightly coupled, but they sit in two different specialties that rarely talk. Headache neurologists treat the attacks. Gynecologists and HRT clinicians manage the hormones. Many women fall in the gap, and many end up on years of preventive migraine medications that miss the underlying hormonal driver entirely.
The 2026 picture is clearer than it has been in decades, and it points in a different direction than most women have been told. The lever is hormonal stability, delivered through transdermal estradiol and continuous progesterone, dosed at the minimum effective level. Done correctly, HRT is not a migraine risk -- it is often part of the migraine fix.
How Estrogen Drives Migraine
Migraine is fundamentally a sensitivity-of-brain disorder, and estrogen is one of the most powerful modulators of that sensitivity. Estrogen affects serotonin signaling, vascular tone, cortical excitability, and the trigeminal nociceptive system that generates migraine pain.
The clinically relevant pattern is not "high estrogen bad, low estrogen good." It is "estrogen change triggers attacks." Specifically:
- Estrogen withdrawal -- a sharp drop from a higher to a lower level -- is the most consistent trigger. This is why classic menstrual migraine attacks cluster in the 2 days before and the first 3 days of menstruation, when premenstrual estrogen falls steeply [1].
- High estrogen surges -- particularly in the late follicular phase or with supraphysiologic dosing from combined oral contraceptives -- can trigger aura by lowering the cortical-spreading-depression threshold.
- Stable estrogen -- whether high or low -- is generally protective. Women with regular cycles who become pregnant often experience dramatic improvement in the second and third trimesters, when estrogen levels are high but stable.
Perimenopause is the worst possible scenario for hormonal migraine because it produces the largest swings of any reproductive life stage. Estradiol can spike to twice premenopausal peak levels and crash to postmenopausal lows within the same cycle. The result is repeated estrogen withdrawals at unpredictable intervals -- the exact stimulus pattern that generates migraine.
The Perimenopausal Worsening Pattern
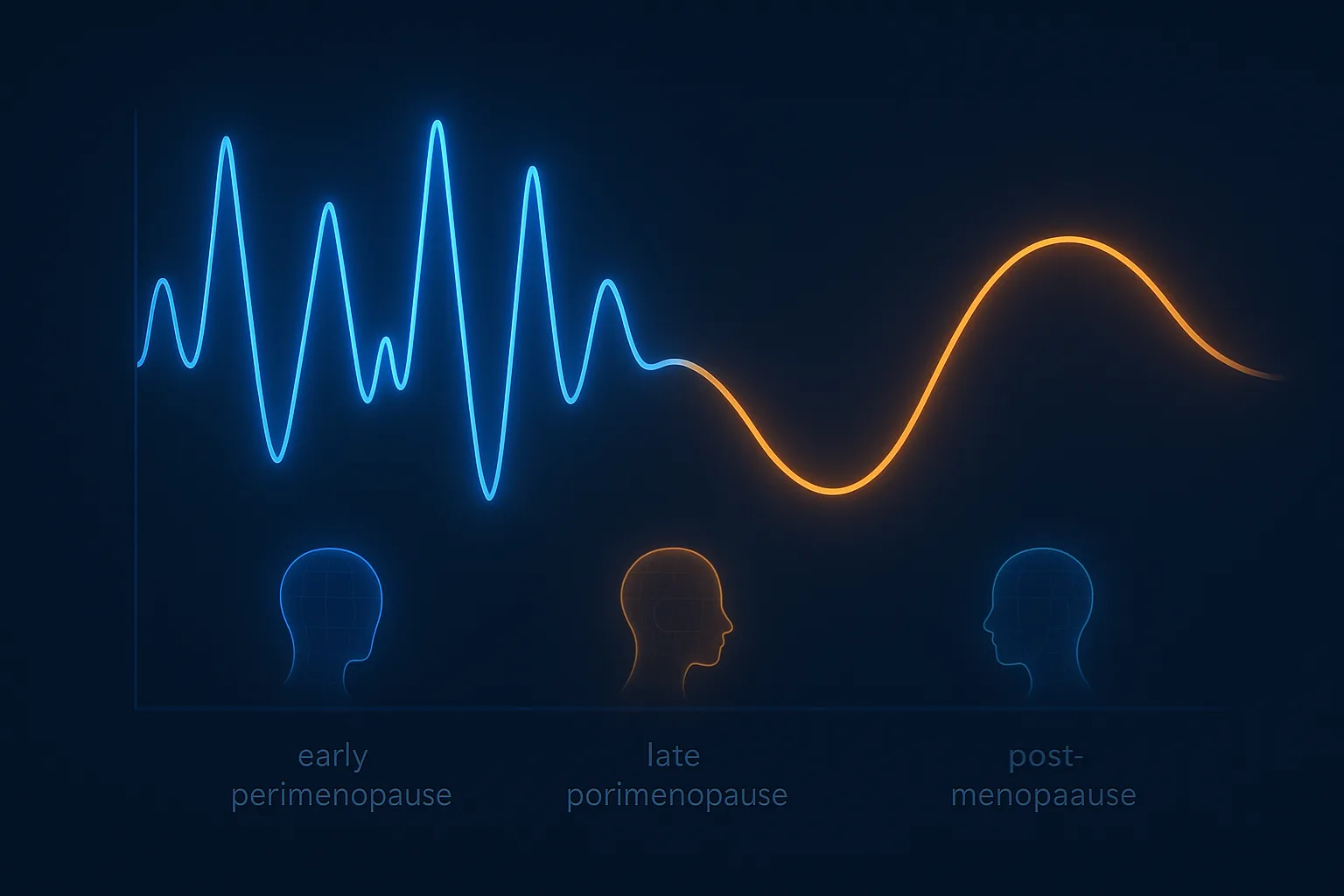
Most women with prior hormonal migraine experience a defined arc through the menopausal transition:
- Early perimenopause: Cycles shorten, late luteal estrogen drops accelerate, attack frequency starts climbing
- Late perimenopause: Cycles become irregular, estrogen swings become extreme, attack frequency peaks
- Final menstrual period and early menopause: Estrogen stabilizes at a low level; attack frequency typically improves
- Established postmenopause: Most women see migraine frequency drop below pre-perimenopausal baseline
About two-thirds of women with prior migraine see worsening during late perimenopause. About half of women report substantial improvement in postmenopause [2]. The middle stage -- the 1 to 3 years of late perimenopause -- is the worst, and it is also the stage when women most often present for HRT consultation.
Why Oral and Transdermal HRT Are Different
The single most important formulation decision in migraine HRT is route of delivery. Oral and transdermal estrogen produce fundamentally different pharmacokinetic profiles, and the difference matters for migraine.
Oral Estrogen: Peaks, Troughs, and First-Pass Liver Effects
Swallowed estrogen is absorbed through the gut and travels first to the liver via the portal circulation. The liver does several things that make oral estrogen problematic for migraine:
- First-pass metabolism produces variable peak levels. Estradiol peaks within hours of dosing, then drops over 24 hours -- a daily peak-and-trough cycle that can mimic estrogen withdrawal.
- Hepatic protein synthesis is upregulated. Oral estrogen increases sex hormone-binding globulin (SHBG), thyroxine-binding globulin, angiotensinogen, and -- critically -- coagulation factors.
- Clotting factor changes raise thrombotic risk. The increase in clotting factors is the main reason oral estrogens carry a higher venous thromboembolism (VTE) and ischemic stroke risk than transdermal forms.
For migraine sufferers, the daily peak-and-trough pattern is the clinical issue. The same withdrawal-like signal that triggers menstrual migraine can be reproduced every 24 hours by oral estrogen.
Transdermal Estradiol: Steady State and No First-Pass Effects
Patches, gels, and sprays deliver estradiol directly through the skin into the systemic circulation, bypassing the liver. The implications:
- Steady plasma estradiol levels with twice-weekly patches or daily gels -- minimal peak-and-trough variation
- No first-pass liver effect, so SHBG, thyroid binding, and coagulation factors stay closer to baseline
- Lower VTE and ischemic stroke risk compared to oral, with multiple cohort studies showing no excess risk for transdermal vs no HRT [3]
- Lower triglyceride and inflammatory marker effects, which matters in metabolically vulnerable women
For migraine specifically, the steady-state pharmacokinetics of transdermal estradiol are the main therapeutic feature. You are removing the daily withdrawal signal that oral dosing creates.
What Current Guidelines Say
Major societies converge on transdermal estradiol as first-line HRT for women with migraine:
- British Menopause Society (2026 update): Use the lowest dose of transdermal estradiol that controls vasomotor symptoms [4]
- The Menopause Society: Transdermal preferred for women with migraine, particularly migraine with aura
- International Headache Society: Migraine with aura does not contraindicate physiologic transdermal estrogen replacement
- European Headache Federation: Combined oral contraceptives contraindicated in migraine with aura; transdermal HRT not equivalent in risk
The doctrinal split between contraceptive estrogens and HRT estrogens is the key concept. Combined oral contraceptives use ethinylestradiol at doses that are 5 to 10 times higher than physiologic. HRT uses body-identical estradiol at doses that approximate normal premenopausal cycling. The two are not pharmacologically interchangeable, even though both are "estrogen."
The Aura Question
Migraine with aura is a known risk factor for ischemic stroke -- approximately 2 to 3 times the baseline risk in women under 50 [5]. The risk increases substantially with smoking and combined oral contraceptive use. This is why combined oral contraceptives are contraindicated in women with migraine with aura.
The question for HRT is whether body-identical transdermal estradiol carries the same risk as combined oral contraceptives. The answer, based on contemporary cohort and case-control data, is no:
- Transdermal estradiol does not increase ischemic stroke risk in observational studies
- The thrombotic risk of oral HRT is intermediate between transdermal HRT and combined oral contraceptives
- The supraphysiologic ethinylestradiol in oral contraceptives is the main driver of stroke risk in migraine-with-aura, not estrogen exposure per se
Practical guidance for women with migraine with aura who need HRT:
- Use transdermal estradiol at the lowest effective dose
- Avoid oral estrogens unless transdermal is impossible
- Use continuous combined progesterone (avoiding the cyclic withdrawal patterns)
- Address modifiable stroke risk factors -- smoking, hypertension, diabetes, dyslipidemia
- Reassess if aura pattern changes -- new aura, prolonged aura, or aura without subsequent headache should prompt re-evaluation
The framework that most experienced HRT clinicians follow: migraine with aura is a yellow flag for HRT, not a red flag. It changes the formulation choice, not the decision to treat.
Building a Migraine-Aware HRT Protocol
The architectural goal of a migraine-aware HRT protocol is to deliver stable, low-dose, body-identical hormones with the fewest possible fluctuations. The components:
Estrogen: Form, Route, Dose
- Body-identical estradiol rather than conjugated equine estrogens or synthetic estrogens
- Transdermal route -- patch, gel, or spray -- rather than oral
- Lowest dose that controls vasomotor symptoms. Typical starting dose: 25 to 50 mcg/day patch, 0.5 to 1.0 mg/day gel, or one to two spray pumps daily
- Twice-weekly patches generally produce more stable levels than once-weekly patches; daily gels and sprays produce the steadiest curves
The estradiol dose that controls hot flashes is usually the dose that controls hormonal migraine. Higher doses do not produce better migraine outcomes and may worsen them in some women.
Progesterone: Continuous, Body-Identical
- Continuous (not cyclic) regimen. Daily progesterone every day -- no monthly withdrawal bleeds
- Micronized progesterone at 100 to 200 mg/day, taken at bedtime, is generally better tolerated than synthetic progestins for migraine
- Levonorgestrel IUD is an alternative that provides endometrial protection with minimal systemic progestin exposure -- a strong option for migraine-prone women who tolerate IUDs
- Continuous combined transdermal patches (estradiol plus progestin together) are simpler but limit dose flexibility
If a woman has had a hysterectomy, progesterone is not required for endometrial protection -- but small amounts may still help with sleep and mood, especially for migraine sufferers who are sensitive to hormonal change.
Testosterone: The Often-Forgotten Component
Testosterone is not first-line therapy for migraine, but women with low free testosterone often have broader symptom clusters that overlap with migraine: fatigue, low mood, joint pain, sleep disruption, and reduced exercise tolerance. These symptoms in turn worsen migraine frequency and severity.
For women already on appropriately dosed estrogen and progesterone but who continue to have residual symptoms -- particularly fatigue, low libido, or joint pain alongside migraine -- adding low-dose testosterone cream or gel for women is consistent with the Global Consensus Position Statement on testosterone therapy for women [6]. It is not a migraine treatment per se, but it can shift the broader physiologic substrate that migraine sits on.
For women weighing combined hormone therapy, comprehensive women's clinics that handle estradiol, progesterone, and testosterone together produce better outcomes than fragmented care. See Best Online HRT Clinics for Women for clinics offering full evaluation rather than treating each hormone in isolation.
What to Expect on Treatment
The First 8 Weeks
The first 4 to 8 weeks of HRT can be rocky for migraine sufferers. The hormonal environment is shifting from whatever pattern was present (often perimenopausal chaos or postmenopausal estrogen depletion) to a new steady state. Some women feel worse before they feel better.
Common patterns in the first 8 weeks:
- No change. The most common pattern. The body is adjusting to the new dose and the migraine baseline has not yet shifted.
- Slightly worse. Some women experience a transient uptick in attack frequency for 4 to 8 weeks, particularly when starting at higher doses or when transitioning off cyclic to continuous progesterone.
- Better immediately. Less common but real, especially in late-perimenopausal women whose estrogen is crashing rapidly.
- Significantly worse and not improving. This is a signal that the formulation, route, or dose is wrong. It is not a signal that HRT is wrong.
The recommended approach: pick a starting dose, hold it stable for 8 to 12 weeks, then assess. Avoid frequent dose changes -- they reproduce exactly the hormonal instability that drives migraine in the first place.
What Improvement Looks Like
For responders, the improvement pattern is gradual:
- Months 2 to 3: Attack frequency starts to drop. Severity often improves before frequency does.
- Months 3 to 6: Stable new baseline emerges. Many women see attack frequency cut in half.
- Months 6 to 12: Sustained improvement. Some women come off preventive migraine medications they have been on for years.
Acute migraine medications (triptans, gepants, NSAIDs) remain available throughout. HRT is a preventive intervention that works alongside, not instead of, acute treatment.
When HRT Is Not the Right Migraine Tool
HRT is not appropriate for every woman with menopausal migraine. Situations where HRT is not the primary lever:
- Migraine with truly atypical features -- prolonged aura over 60 minutes, hemiparesis, brainstem symptoms, or aura without subsequent headache -- requires neurological workup before any hormonal intervention
- High thrombotic risk -- prior VTE, factor V Leiden, antiphospholipid syndrome -- requires individualized risk-benefit assessment
- Estrogen-receptor-positive breast cancer history -- alternative non-hormonal approaches (CGRP antibodies, gepants, lifestyle interventions) take priority
- Rapidly worsening migraine pattern with new neurological signs -- structural causes need to be excluded first
For women in these categories, non-hormonal preventive strategies (CGRP-targeted antibodies, OnabotulinumtoxinA, beta-blockers, anticonvulsants) are first-line. HRT may still be considered, but the decision framework is more individualized.
How Migraine HRT Differs From Standard HRT
Most women starting HRT do not need migraine-specific tuning -- the standard transdermal estradiol plus oral micronized progesterone protocol works for the majority. But for women with prior hormonal migraine, three architectural decisions matter more than they do for typical patients:
- Route is non-negotiable. Oral estrogen is rarely the right choice for a migraine-prone woman.
- Continuous progesterone is preferred over cyclic. Cyclic regimens reproduce the monthly withdrawal that drives menstrual migraine.
- Stability beats potency. A modest dose held stable for months produces better outcomes than aggressive dosing with frequent adjustments.
These decisions are well within the standard practice of a competent HRT clinician, but they require the clinician to ask about migraine history at intake. Many do not. Women with prior migraine should raise this themselves and ensure the protocol reflects it.
For more on hormonal architecture in menopause, see Bioidentical vs Synthetic HRT for Women, which covers the form-and-route decisions in depth. For the broader symptom picture, see Perimenopause Symptoms Timeline.
When to Get a Hormonal Workup
A migraine-aware hormonal evaluation is reasonable if any of the following apply:
- New or worsening migraine in a woman age 40 to 55
- Pre-existing menstrual migraine with deteriorating cycle pattern
- Migraine attacks clustering near vasomotor symptoms (hot flashes, night sweats, mood changes)
- Failed response to standard preventive migraine medications
- Migraine emerging or worsening in the year after surgical menopause
A reasonable workup includes estradiol, FSH, LH, free and total testosterone, SHBG, thyroid function (TSH and free T4), HbA1c, vitamin D, and basic lipid panel. The goal is not just to confirm menopausal status but to establish a baseline for monitoring the response to HRT.
For women with active migraine, a clinician comfortable with both hormonal and headache management is more useful than two separate specialists who do not coordinate. Comprehensive women's HRT clinics that include neurological context -- migraine history, aura subtype, prior preventive medications -- produce better individualized protocols than headache-only or hormone-only practices.
See Best Online HRT Clinic for Women for clinics that handle the full picture rather than punting between specialties.
Bottom Line
Perimenopausal and menopausal migraine is a hormonal-stability problem more than a hormonal-deficiency problem. The most common mistake is treating it as either pure neurology (more triptans, more preventive medications, no hormonal intervention) or pure gynecology (start any HRT, see what happens). The right architecture is migraine-aware HRT: transdermal estradiol at the lowest effective dose, continuous body-identical progesterone, stable dosing held for at least 8 to 12 weeks before reassessment.
For most women, this protocol reduces attack frequency within 3 months without raising stroke or thrombotic risk above baseline. Migraine with aura is not a contraindication to body-identical transdermal HRT, despite being a clear contraindication to combined oral contraceptives. The pharmacology is different, the doses are different, and the risk profile is different.
If you have prior hormonal migraine and are entering perimenopause, treating the hormones early -- before the migraine pattern destabilizes for years -- is generally easier than rescuing a disrupted system later. The clinical lever is steady physiologic estradiol, delivered transdermally, paired with continuous progesterone, at the minimum effective dose.
Related Reading
References
-
MacGregor EA. Migraine, menopause and hormone replacement therapy. Post Reprod Health. 2018;24(1):11-18. PMID: 28994639
-
Pavlovic JM, Allshouse AA, Santoro NF, et al. Sex hormones in women with and without migraine: Evidence of migraine-specific hormone profiles. Neurology. 2016;87(1):49-56. PMID: 27251885
-
Renoux C, Dell'Aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: a nested case-control study. BMJ. 2010;340:c2519. PMID: 20525678
-
British Menopause Society. Tool for Clinicians: Migraine and HRT (April 2026). BMS Migraine and HRT 2026
-
Schurks M, Rist PM, Bigal ME, et al. Migraine and cardiovascular disease: systematic review and meta-analysis. BMJ. 2009;339:b3914. PMID: 19861375
-
Davis SR, Baber R, Panay N, et al. Global Consensus Position Statement on the Use of Testosterone Therapy for Women. J Clin Endocrinol Metab. 2019;104(10):4660-4666. PMID: 31474158
-
Sacco S, Merki-Feld GS, Aegidius KL, et al. Hormonal contraceptives and risk of ischemic stroke in women with migraine: a consensus statement from the European Headache Federation and the European Society of Contraception and Reproductive Health. J Headache Pain. 2017;18(1):108. PMID: 29086160
-
The North American Menopause Society. The 2022 hormone therapy position statement of The North American Menopause Society. Menopause. 2022;29(7):767-794. PMID: 35797481