Perimenopause in Your 30s: What a 4,432-Woman Study Found
6/3/2026
5 min read
By The TRT Catalog
A UVA Health and Flo study found 55% of women aged 30-35 report moderate-to-severe perimenopause symptoms. What it means and how to get evaluated young.
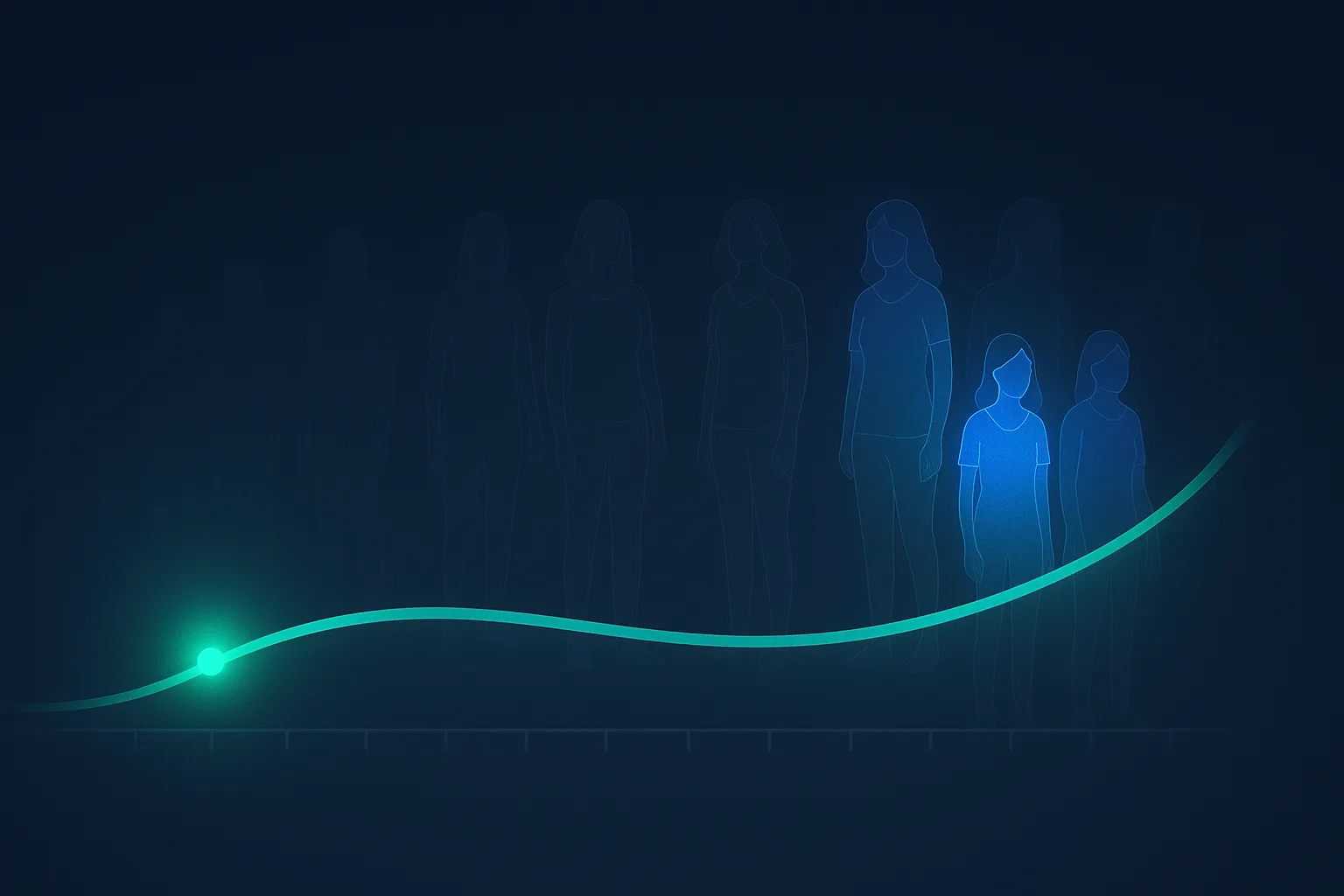
Key Takeaways: A study from UVA Health and Flo Health, published in npj Women's Health, analyzed self-reported symptoms from 4,432 American women aged 30 and older. The headline finding: 55.4% of women aged 30-35 reported menopause-associated symptoms meeting the moderate-or-severe threshold on the validated Menopause Rating Scale, rising to 64.3% in women aged 36-40. The earliest-emerging symptoms were psychological -- anxiety, depressed mood, irritability, low energy -- which peaked around 41-45, while the classic physical symptoms (hot flashes, vaginal dryness, bladder issues) emerged later and peaked after 50. Most women don't seek treatment until 56 or older, despite symptoms beginning decades earlier. The practical takeaway: perimenopause in your 30s is biologically real and far more common than the "menopause happens at 50" script suggests -- and the symptoms most likely to show up early are exactly the ones most likely to be misread as stress, anxiety, or depression.
What the Study Found
Researchers at the University of Virginia Department of Psychiatry and Neurobehavioral Sciences, working with the women's-health app Flo Health, analyzed symptom data self-reported by 4,432 American women aged 30 and older. They scored each woman on the Menopause Rating Scale (MRS) -- a validated, widely used instrument that quantifies the severity of 11 menopause-associated symptoms across psychological, somatic, and urogenital domains. The findings were published in npj Women's Health, with Dr. Jennifer Payne as senior author.
The numbers that drew attention:
55.4% of women aged 30-35 reported symptoms meeting the moderate-or-severe threshold on the MRS
64.3% of women aged 36-40 met that same threshold
Psychological symptoms (anxiety, depressed mood, irritability) emerged earliest and peaked around ages 41-45
Physical and urogenital symptoms (hot flashes, sweating, bladder issues, vaginal dryness) peaked later, after age 50
Most women delay seeking treatment until age 56 or older -- often decades after symptoms begin
The age-related symptom sequence is the part clinicians should internalize. The popular image of menopause is a 50-year-old woman fanning herself through a hot flash. The data says the transition often announces itself a decade or more earlier, and it announces itself through mood and energy, not heat.
Why the Early Symptoms Get Missed
Perimenopause is the hormonal transition that precedes the final menstrual period. It is not a single event; it is a years-long process during which ovarian estradiol and progesterone production becomes erratic -- swinging high and low rather than steadily declining. Those swings are what drive symptoms, and they can begin 8-10 years before the final period. For a woman whose menopause will arrive at 51, that means symptoms can plausibly start at 41 -- and the UVA-Flo data shows a substantial fraction experiencing them even earlier, in the 30-35 band.
The problem is that the earliest symptoms are the ones least likely to be recognized as hormonal:
New or worsening anxiety
Mood swings and irritability
Low or flat energy that sleep doesn't fix
Difficulty concentrating ("brain fog")
Sleep that feels less restorative
Changes in libido
Every one of these overlaps with the symptom profile of an anxiety or depressive disorder, with chronic stress, and with the generic fatigue of a busy life. So they get attributed to those things. A 35-year-old who reports anxiety and low energy to her doctor is far more likely to leave with an SSRI prescription or a "try to manage your stress" than with a perimenopause evaluation -- because perimenopause isn't on the differential for someone that age.
Women's HRT — Menopause-First Telehealth
Bioidentical estradiol, progesterone, and low-dose testosterone — all 50 states, unlimited physician access.
The single most common reason a younger woman gets falsely reassured is a normal hormone panel. Here is why that reassurance is often wrong.
In early perimenopause, FSH and estradiol don't drop in a smooth line. They oscillate -- a woman can have a perfectly normal estradiol on the day of her blood draw and be deep in a symptomatic transition. A single FSH or estradiol value, the standard reflex test, has poor sensitivity for early perimenopause. A "normal" result rules out very little.
Perimenopause is, by current guidance, a clinical diagnosis -- built from the symptom pattern, the menstrual-cycle history, and the timing, not from a single number. Thyroid disease, iron deficiency, sleep disorders, and primary mood disorders should be ruled out because they mimic the picture. But a normal estradiol on one Tuesday is not a reason to close the case in a symptomatic 38-year-old. If a clinician uses one lab value to dismiss the possibility, that is itself a signal to get a second opinion from someone with menopause training.
What Treatment Actually Looks Like at This Age
For a woman in her late 30s or 40s with disruptive perimenopause symptoms and no contraindications, several evidence-based paths exist, and the right one depends on her cycle status, contraceptive needs, and symptom profile.
Stabilize the hormonal swings. The symptoms are driven by fluctuation, so the goal is to smooth it. For some women that means low-dose transdermal estradiol plus oral micronized progesterone (progesterone is needed for uterine protection in women with a uterus). For women who also need contraception, a low-dose hormonal contraceptive can flatten the swings and treat symptoms simultaneously -- a frequently overlooked option in this exact age band.
Layer in testosterone where it fits. Persistent low energy, low mood, and reduced libido that survive the estrogen-progesterone base are often the signature of the androgen side of the transition. Low-dose testosterone -- typically a 5 mg/day cream or a small weekly injection -- is sometimes added for these residual symptoms. There is no FDA-approved testosterone product for women in the US, so this is prescribed off-label by clinicians experienced in women's hormone therapy. Our testosterone for perimenopause writeup covers the dosing logic and what to expect.
The timing hypothesis favors you. Younger age is generally a favorable factor in the hormone-therapy risk-benefit calculation. The timing hypothesis -- the principle that hormone therapy started earlier in the transition carries a more favorable cardiovascular and cognitive profile than therapy started a decade past menopause -- means a symptomatic 40-year-old is, if anything, in the most favorable window to consider treatment, not the least.
The point is not that every symptomatic 35-year-old needs hormones. It's that the option should be on the table and evaluated, rather than foreclosed because of a calendar age that the biology doesn't actually respect.
How to Get Evaluated If You Think This Is You
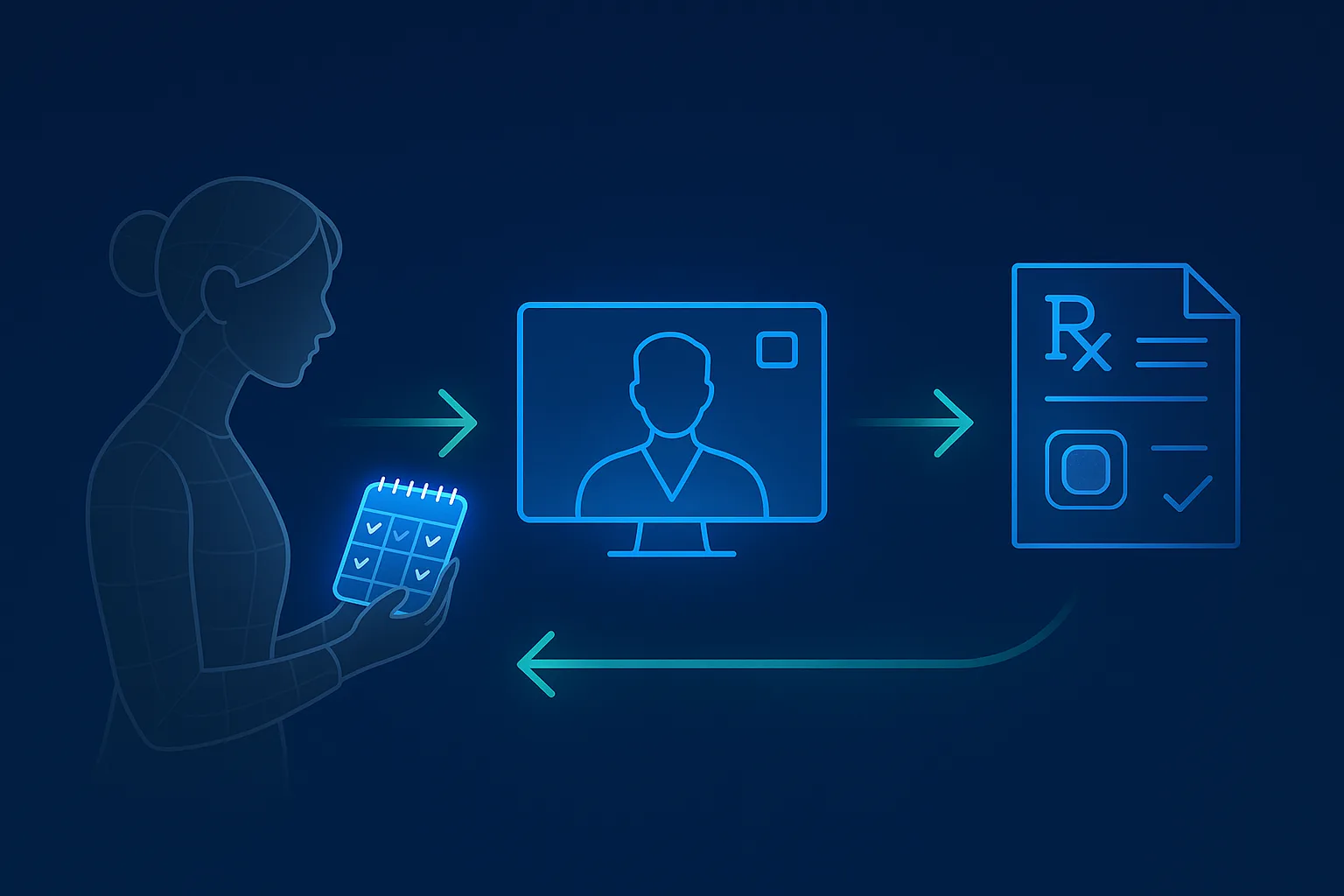
The UVA-Flo data is, at the individual level, a permission slip: if you are in your 30s or early 40s and something hormonal feels off, you are not imagining it and you are not too young. The practical sequence:
Track for 2-3 months. Log symptoms, rate severity 1-10, and note timing relative to your cycle. Cycle changes -- shorter, longer, heavier, lighter, skipped -- are useful corroborating data even though they aren't required for diagnosis.
Raise it directly. At your next visit: "I think I may be in early perimenopause. Can we evaluate that specifically and discuss options?" Naming it puts it on the differential, which is half the battle.
Don't accept a single normal lab as a closed case. If your only basis for "you're fine" is one estradiol or FSH draw, ask about the limitation of single-point testing in early perimenopause.
Find menopause-trained care if you hit a wall. The Menopause Society practitioner directory (menopause.org/find-a-menopause-practitioner) filters for clinicians with the MSCP credential. If your symptoms are predominantly psychological and you've already been routed to a mood-disorder pathway, a menopause-trained second opinion is worth the friction.
Consider a women's HRT telehealth clinic. Well-run platforms screen for perimenopause proactively at intake and prescribe the modern transdermal estradiol + progesterone (+ testosterone where indicated) protocol as a default rather than a niche request. The trade-off is that quality varies widely. Our best online HRT clinic for women comparison grades platforms on diagnostic rigor, protocol depth, clinician training, and pricing transparency -- the differences meaningfully affect whether you get evaluated properly or just sold a product.
What the Study Doesn't Resolve
A few honest limitations:
Self-reported, app-based sample. The data comes from women using the Flo app, who skew younger, more health-engaged, and more symptom-aware than the general population. The MRS captures symptom burden, not a formal perimenopause diagnosis -- a high MRS score in a 32-year-old could reflect perimenopause, but it could also reflect a thyroid disorder, a mood disorder, or another cause that the survey design can't disentangle.
Cross-sectional, not longitudinal. The study captures symptom prevalence by age group at one point; it doesn't follow individual women through the transition.
No biochemical confirmation. Symptoms were scored without paired hormone testing, so the study establishes that young women report substantial symptom burden -- not that all of that burden is hormonally driven perimenopause.
None of this undercuts the central, useful finding: a large fraction of women in their 30s are carrying a moderate-to-severe, menopause-pattern symptom load, the symptoms skew psychological and early, and the care system is not set up to recognize it at that age. The limitations sharpen the action item rather than weaken it -- if you fit the picture, the move is a proper evaluation that rules out the mimics and takes early perimenopause seriously as a possibility.
The Bottom Line
The UVA Health and Flo Health study puts a number on something many women in their 30s have felt and been told to ignore: more than half of women aged 30-35, and nearly two-thirds aged 36-40, report moderate-to-severe menopause-associated symptoms. The earliest of those symptoms are anxiety, mood swings, low energy, and brain fog -- the exact symptoms most likely to be filed under "stress" or "depression" and never connected to the hormonal transition driving them.
Perimenopause in your 30s is biologically plausible, statistically common, and frequently missed. The fix is not to assume every symptomatic young woman is perimenopausal -- it's to put the possibility on the table, evaluate it properly, rule out the mimics, and recognize that a single normal lab value doesn't close the case. The treatments exist, the timing window is favorable, and the friction to getting evaluated is lower than it has ever been.
References
Payne JL, et al. Perimenopause symptoms, severity, and healthcare seeking in women in the US. npj Women's Health. 2025. DOI: 10.1038/s44294-025-00061-3.
UVA Health. Young Women Suffering Menopause Symptoms in Silence, Study Reveals. February 2025.
The 2022 hormone therapy position statement of The North American Menopause Society. Menopause. 2022;29(7):767-794.
Harlow SD, Gass M, Hall JE, et al. Executive summary of the Stages of Reproductive Aging Workshop +10 (STRAW+10). J Clin Endocrinol Metab. 2012;97(4):1159-1168.
Santoro N. Perimenopause: From Research to Practice. J Womens Health. 2016;25(4):332-339.
Yes. The UVA Health and Flo Health study published in npj Women's Health found that 55.4% of women aged 30-35 reported menopause-associated symptoms that met the 'moderate' or 'severe' threshold on the validated Menopause Rating Scale, rising to 64.3% in women aged 36-40. Perimenopause -- the hormonal transition before the final period -- can begin 8-10 years before menopause itself, which means symptoms in the mid-to-late 30s are biologically plausible, not premature. The hallmark early symptoms in younger women are psychological (anxiety, mood swings, irritability, low energy) rather than the hot flashes most people associate with menopause, which is precisely why they get misattributed to stress, depression, or 'just life.'
What are the early signs of perimenopause in your 30s?
In the UVA-Flo data, the earliest-emerging symptoms were psychological: anxiety, depressed mood, irritability, and reduced energy and concentration. These peaked around ages 41-45. Physical symptoms -- night sweats, sleep disruption, joint aches, vaginal dryness, bladder changes, and the classic hot flashes -- tend to emerge later and peak after 50. Irregular or changing menstrual cycles can accompany the early phase but are not required for a perimenopause diagnosis. The practical signature in a 35-year-old is new or worsening anxiety and mood instability, unexplained fatigue, sleep that isn't as restorative, and a sense that 'something hormonal' shifted -- often dismissed by both the woman and her doctor as too-young-to-be-menopause.
How is perimenopause diagnosed in a younger woman?
Perimenopause is a clinical diagnosis based on symptoms and menstrual-cycle changes, not a single blood test. FSH and estradiol fluctuate dramatically day to day in early perimenopause, so a 'normal' result on any given day does not rule it out -- this is the most common reason younger women get falsely reassured. A good evaluation reviews symptom pattern, cycle history, and timing, rules out thyroid disease and other mimics, and may use serial labs rather than a single draw. The Menopause Rating Scale or Greene Climacteric Scale can quantify symptom burden. If a clinician dismisses the possibility purely on age or one lab value, that is a reason to seek a menopause-trained provider.
Is hormone therapy appropriate for perimenopause in your 30s?
It can be, and the decision is individualized. For women in their late 30s and 40s with disruptive perimenopause symptoms and no contraindications, low-dose transdermal estradiol plus oral micronized progesterone (for women with a uterus) is an evidence-based option to stabilize the hormonal swings driving mood, sleep, and vasomotor symptoms. Some women in this window do well on a hormonal contraceptive that smooths the fluctuations instead. Low-dose testosterone is sometimes layered in for persistent energy, mood, and libido complaints. Younger age is generally favorable for the risk-benefit calculus -- the 'timing hypothesis' shows hormone therapy started earlier in the transition carries a more favorable profile than therapy started a decade past menopause.
Why do doctors miss perimenopause in younger women?
Three reasons. First, the cultural script says menopause happens around 50, so both patients and clinicians assume a 35-year-old is 'too young' and look for other explanations. Second, the early symptoms are psychological and overlap heavily with anxiety and depression, so they get treated as a primary mood disorder rather than a hormonal one. Third, a single normal FSH or estradiol level -- which is common in early perimenopause because the hormones swing rather than steadily decline -- is used to rule it out. The UVA researchers explicitly flagged this pattern: women in their 30s suffering in silence because the diagnosis isn't on anyone's radar.
What should I do if I think I'm perimenopausal in my 30s?
Track your symptoms and cycle for 2-3 months, rate severity, and note timing relative to your period. Raise it directly at your next visit: 'I think I may be in early perimenopause -- can we evaluate that and discuss options?' If your primary care or OB/GYN is dismissive on age alone, find a Menopause Society-certified practitioner (directory at menopause.org) or use a women's HRT telehealth clinic that screens for perimenopause proactively. Our breakdown of the best online HRT clinics for women grades platforms on diagnostic rigor and protocol depth so you can avoid the marketing-only operations.