Women lose up to 20% of bone density in the 5-7 years after menopause. HRT cuts fracture risk 24-34%. When to start, DEXA timing, and what the data shows.
Key Takeaways: Women can lose up to 20% of their bone density in the 5-7 years following menopause. Estrogen deficiency is the primary driver of this loss. The Women's Health Initiative proved that HRT reduces fracture risk by 24-34% and increases bone mineral density at the hip and spine. Testosterone adds additional bone-building effects that estrogen alone does not provide. Starting HRT early in menopause -- when bone loss is fastest -- offers the strongest protection.
Menopause Is a Bone Emergency Most Women Do Not See Coming
Osteoporosis does not announce itself. There is no pain, no obvious symptom, no warning before a vertebra collapses or a hip fractures from a minor fall. By the time a woman gets diagnosed, she has often already lost significant bone mass.
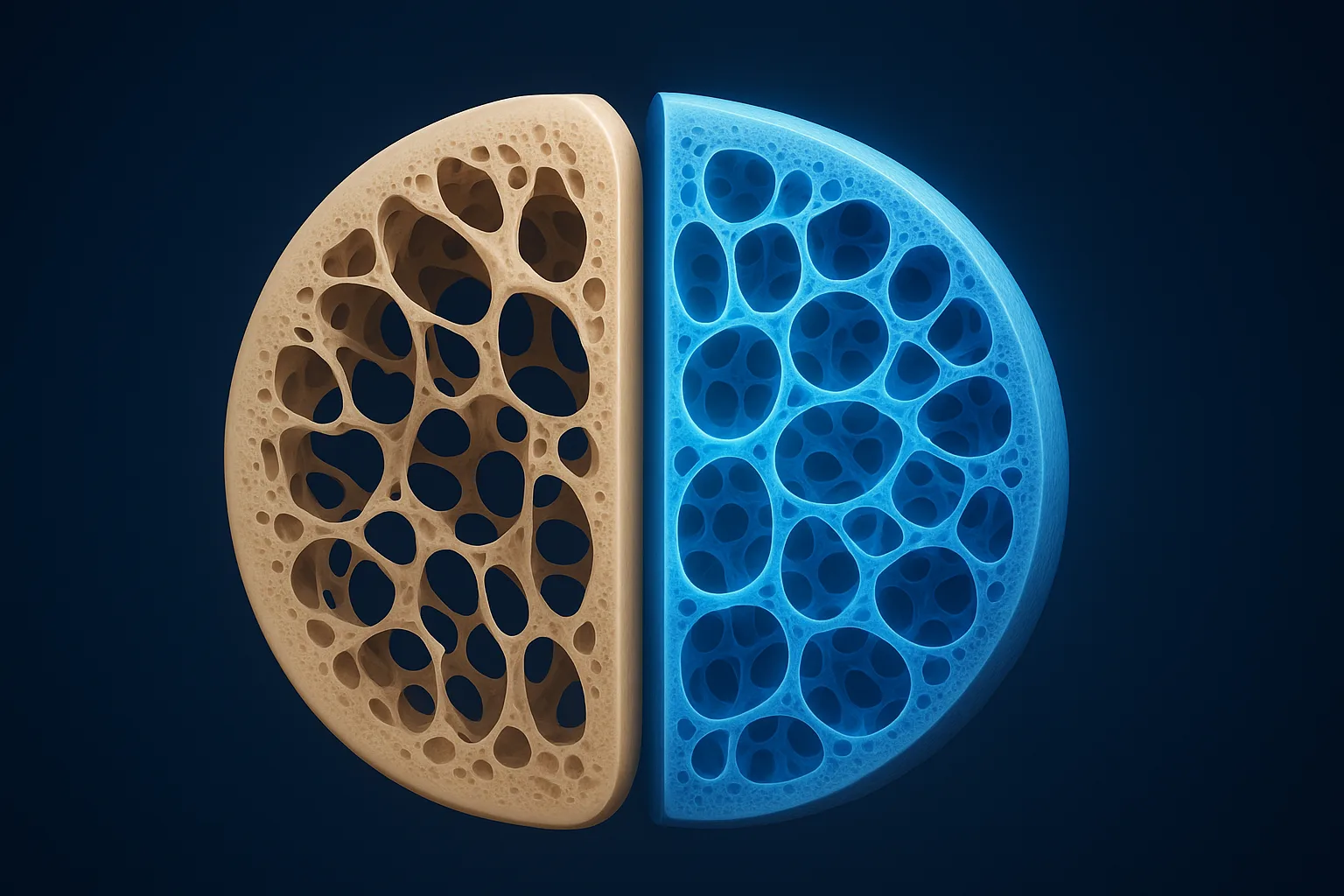
Here is the timeline most women are not told about: bone loss accelerates sharply at menopause and stays elevated for 5-7 years. During this window, trabecular bone (the spongy interior of vertebrae and the ends of long bones) can decline at rates of 3-5% per year [1]. Over the full menopausal transition, total bone mineral density losses of 10-20% are common across the spine, hip, and forearm.
This is not a slow, gentle decline. It is a structural crisis that happens during the same years many women are managing hot flashes, sleep disruption, and mood changes -- and bone loss gets almost no attention compared to those visible symptoms.
One in two women over 50 will break a bone due to osteoporosis in her remaining lifetime. Hip fractures carry a 20% mortality rate in the first year. These are not abstract statistics. They represent the downstream consequence of untreated estrogen deficiency on the skeleton.
How Estrogen Protects Bone
Understanding why menopause destroys bone requires understanding estrogen's role in bone remodeling -- the continuous cycle of bone breakdown and rebuilding that keeps the skeleton healthy.
The Remodeling Cycle
Bone is not static. Your body constantly removes old bone (resorption) and replaces it with new bone (formation). Two cell types run this process:
Osteoclasts break down old or damaged bone
Osteoblasts build new bone to replace what was removed
In premenopausal women, these processes are roughly balanced. You break down about as much bone as you build. Estrogen is the master regulator that maintains this balance [3].
What Estrogen Does at the Cellular Level
Estrogen acts on bone through multiple mechanisms:
Suppresses osteoclast formation and activity. Estrogen inhibits the differentiation of osteoclast precursor cells, reducing the number of active bone-resorbing cells. It also shortens the lifespan of mature osteoclasts by promoting apoptosis (programmed cell death) [3].
Supports osteoblast function. Estrogen enhances the activity of bone-building osteoblasts, promoting mineralization and the production of bone matrix proteins.
Regulates inflammatory cytokines. Estrogen suppresses IL-1, IL-6, and TNF-alpha -- inflammatory signaling molecules that stimulate osteoclast formation. When estrogen drops at menopause, these cytokines surge, creating a pro-resorptive environment [3].
Modulates calcium absorption. Estrogen promotes intestinal calcium absorption and reduces renal calcium excretion, keeping more calcium available for bone mineralization.
The Menopausal Collapse
When estrogen levels fall at menopause, every one of these protective mechanisms fails simultaneously:
Osteoclast numbers and activity increase dramatically
Osteoblast function declines
Inflammatory cytokines surge
Calcium absorption drops
The result is a remodeling imbalance where bone breakdown far outpaces bone formation. The body is literally dissolving its own skeleton faster than it can rebuild it. This accelerated phase lasts 5-7 years before bone loss eventually slows to a lower (but still negative) rate [1].
The Women's Health Initiative: The Definitive Bone Data
The Women's Health Initiative (WHI) remains the largest randomized controlled trial of hormone therapy ever conducted. While it is most often discussed in the context of cardiovascular and breast cancer risk, its bone data is unequivocal.
What the WHI Proved
The estrogen-plus-progestin arm of the WHI enrolled 16,608 postmenopausal women aged 50-79. After an average follow-up of 5.6 years [2]:
Outcome
Reduction with HRT
Total fractures
24% reduction (HR 0.76)
Hip fractures
34% reduction (HR 0.66)
Vertebral fractures
34% reduction (HR 0.66)
Spine BMD increase
+4.5% at 3 years
Hip BMD increase
+3.7% at 3 years
The estrogen-only arm (in women who had undergone hysterectomy) showed similar fracture protection, with a 30-39% reduction in hip fracture risk [2].
What Makes This Data So Strong
The WHI bone findings are remarkable for several reasons:
Universal benefit. Fracture reduction occurred regardless of baseline bone density, age at enrollment, body weight, or fall risk. Women who were not classified as osteoporotic at baseline still benefited [2].
Durable effect. Follow-up analyses showed that significant hip fracture protection persisted over 13 years for women assigned to combined hormone therapy.
Dose-dependent. Even low-dose estrogen regimens (0.3mg conjugated estrogen or equivalent) have been shown to prevent bone loss, though standard doses provide the most robust protection [5].
HRT is the only intervention proven to reduce fractures at all skeletal sites in a large randomized trial. No bisphosphonate trial has demonstrated this breadth of protection.
Women's HRT — Menopause-First Telehealth
Bioidentical estradiol, progesterone, and low-dose testosterone — all 50 states, unlimited physician access.
Estrogen gets most of the attention in the bone density conversation, but testosterone plays a distinct and complementary role. This is relevant because testosterone levels also decline significantly around menopause -- by roughly 50% compared to peak levels in the mid-20s.
How Testosterone Builds Bone
Testosterone acts on bone through mechanisms that do not overlap entirely with estrogen:
Direct androgen receptor stimulation. Osteoblasts express androgen receptors. Testosterone binding to these receptors directly stimulates bone formation -- a pathway estrogen does not activate [4].
Periosteal bone growth. Testosterone promotes expansion of the outer bone surface (periosteum), increasing bone diameter and mechanical strength. Estrogen does not have this effect. Larger bone diameter translates to greater resistance to fracture even at the same density.
Muscle-bone interaction. Testosterone maintains muscle mass and strength. Stronger muscles exert greater mechanical loading on bone, which stimulates bone formation through mechanotransduction. This indirect pathway is significant -- sarcopenia (muscle loss) and osteoporosis frequently co-occur in postmenopausal women.
The Evidence for Combined Therapy
A landmark study by Davis et al. demonstrated that combined estradiol and testosterone implants produced significantly greater bone mineral density gains at the hip and spine compared to estradiol alone in postmenopausal women [4].
More recent observational data confirms a positive association between serum testosterone levels and lumbar spine bone mineral density in postmenopausal women, independent of estradiol levels. Free testosterone has been identified as an independent predictor of bone density at the lumbar spine.
The 2019 Global Consensus Position Statement on testosterone therapy for women acknowledged these musculoskeletal benefits, though it noted that the evidence base for bone-specific outcomes needs further randomized trial data [7].
Practical Implications
For women on HRT who still show suboptimal bone density gains, adding physiological-dose testosterone (typically 5-10mg/day via transdermal cream) may provide additional skeletal protection. This is particularly relevant for women with low testosterone levels who also report fatigue, reduced muscle mass, or low libido -- symptoms that share underlying mechanisms with bone loss.
Timing matters more for bone than for almost any other HRT benefit. The reason is straightforward: preventing bone loss is far more effective than trying to rebuild bone after it is gone.
The Window of Opportunity
The fastest bone loss occurs in the first 5-7 years after menopause. Starting HRT during this window prevents the steepest decline. Delaying HRT by even a few years means accepting irreversible structural damage to trabecular bone architecture that no treatment can fully restore.
Within 5 years of menopause: HRT preserves the most bone. Women who start early maintain bone density near premenopausal levels at protected sites.
5-10 years after menopause: HRT still increases BMD and reduces fracture risk, but some structural damage has already occurred. Benefit is still significant.
More than 10 years after menopause: HRT can still improve BMD, but starting de novo hormone therapy solely for bone protection at this stage is less common. Providers often prefer bisphosphonates for women in this category due to the cardiovascular risk-benefit profile shifting with age.
Who Should Prioritize Early HRT for Bone
Every postmenopausal woman loses bone. But some women are at higher risk and should prioritize bone protection in their HRT decision-making:
Early menopause (before age 45, whether natural or surgical) -- longer lifetime estrogen deficiency
Family history of osteoporosis or hip fracture -- genetic predisposition to low peak bone mass
Low body weight (BMI under 20) -- less mechanical loading on bone, lower peripheral estrogen production
Smoking -- directly toxic to osteoblasts and accelerates estrogen metabolism
History of eating disorders -- may have achieved lower peak bone mass
Long-term corticosteroid use -- inhibits bone formation
Sedentary lifestyle -- reduced mechanical loading
Women with early or surgical menopause should strongly consider HRT at minimum until the average age of natural menopause (51) for bone protection alone, regardless of other symptoms [5].
Dual-energy X-ray absorptiometry (DEXA) is the gold standard for measuring bone mineral density and diagnosing osteoporosis. Understanding when and how to use DEXA scanning is essential for making informed HRT decisions.
Current Screening Guidelines
The U.S. Preventive Services Task Force (USPSTF) recommends [6]:
All women age 65 and older: Routine DEXA screening
Postmenopausal women under 65 with risk factors: Screening based on clinical risk assessment (using tools like FRAX)
The American Association of Clinical Endocrinologists (AACE) recommends a lower threshold, suggesting DEXA for all postmenopausal women with risk factors and all women over 50 who have experienced a fracture [6].
Reading Your DEXA Results
DEXA reports two key scores:
T-score compares your bone density to a healthy 30-year-old woman at peak bone mass:
T-Score
Classification
Above -1.0
Normal
-1.0 to -2.5
Osteopenia (low bone mass)
Below -2.5
Osteoporosis
Below -2.5 with fracture
Severe osteoporosis
Z-score compares your density to women your own age. A Z-score below -2.0 suggests bone loss beyond what is expected for your age and warrants investigation for secondary causes.
DEXA Timing for Women on HRT
If you are starting HRT partly for bone protection:
Baseline DEXA at or near the start of treatment (ideally within the first year of menopause)
Follow-up DEXA at 2 years to confirm treatment response
Ongoing monitoring every 2-3 years if stable; annually if density is declining despite treatment
DEXA measures density at two primary sites: the lumbar spine (L1-L4) and the proximal femur (total hip and femoral neck). Both sites should be measured at each visit for comprehensive assessment.
HRT vs. Bisphosphonates: Choosing the Right Approach
Bisphosphonates (alendronate, risedronate, zoledronic acid) are the most commonly prescribed medications for osteoporosis. But they are not the only option, and for many menopausal women, they may not be the best first choice.
Breast tenderness, bleeding (if cyclic), small increased breast cancer risk with combined therapy
GI irritation, jaw osteonecrosis (rare), atypical fractures (rare)
Best candidate
Recently menopausal women with symptoms
Older women, women who cannot take HRT
When HRT Is the Better First Choice
For women within 10 years of menopause who also have vasomotor symptoms (hot flashes, night sweats), HRT is often the logical first-line therapy for bone protection because [5]:
It treats the root cause of menopausal bone loss (estrogen deficiency)
It provides bone protection equivalent to bisphosphonates
It simultaneously treats symptoms that impair quality of life
It avoids the GI side effects common with oral bisphosphonates
When Bisphosphonates Make More Sense
Bisphosphonates are preferred when:
The woman is more than 10 years past menopause
There are contraindications to HRT (history of estrogen-receptor-positive breast cancer, active thromboembolic disease)
The primary goal is bone protection without need for symptom management
Severe osteoporosis requires the strongest possible antiresorptive effect
Combination Therapy
For women with severe osteoporosis or those who continue to lose bone on HRT alone, combining HRT with a bisphosphonate produces additive BMD gains at the hip and spine. However, most women do not need both, and combination therapy is reserved for high-risk cases.
Building a Complete Bone Protection Strategy
HRT is the foundation, but bone health requires a multi-pronged approach. Here is what the evidence supports:
Resistance Training
Weight-bearing and resistance exercise is the single most important non-pharmacological intervention for bone density. Mechanical loading stimulates osteoblasts directly through mechanotransduction.
Resistance training 2-3x per week targeting major muscle groups
Impact exercise (walking, jogging, stair climbing) for hip and spine loading
Balance training to reduce fall risk -- preventing falls prevents fractures
Calcium and Vitamin D
These are necessary but not sufficient on their own:
Calcium: 1,000-1,200mg daily from diet plus supplements if needed. Dairy, sardines, leafy greens, and fortified foods are the best sources.
Vitamin D: 1,000-2,000 IU daily (or more if deficient). Target serum 25(OH)D levels of 30-50 ng/mL. Vitamin D is essential for calcium absorption.
Protein
Adequate protein intake (1.0-1.2g per kg body weight daily) supports both muscle mass and bone matrix formation. Many postmenopausal women are protein-deficient.
Lifestyle Factors
Stop smoking -- smoking directly impairs osteoblast function and accelerates estrogen metabolism
Limit alcohol -- more than 2 drinks daily increases fracture risk
Maintain healthy body weight -- being underweight is a significant osteoporosis risk factor
Monitoring Your Bone Health on HRT
Once you start HRT for bone protection, ongoing monitoring ensures you are getting the expected benefit:
DEXA scans every 2 years to track BMD trends. Look for stable or increasing T-scores at the spine and hip.
Bone turnover markers (optional but useful): serum CTX (C-terminal telopeptide) and P1NP (procollagen type 1 N-terminal propeptide) can show whether bone remodeling has normalized within 3-6 months -- much faster feedback than waiting 2 years for a repeat DEXA.
Vitamin D levels checked annually. Maintain 25(OH)D above 30 ng/mL.
Calcium intake assessment at each visit. Most women need to track their dietary calcium for a week to know whether supplementation is necessary.
If DEXA shows continued bone loss despite HRT, investigate potential causes: vitamin D deficiency, thyroid disease, celiac disease, medication effects (PPIs, corticosteroids), or inadequate HRT dosing. Adding testosterone or a bisphosphonate may be appropriate in refractory cases.
What Happens If You Stop HRT
This is a critical consideration. Bone protection from HRT is not permanent. When you stop taking estrogen, bone loss resumes -- and it resumes at the accelerated menopausal rate, not the slower age-related rate.
Studies show that fracture risk returns to baseline within 2-5 years of stopping HRT. The bone you preserved during treatment is gradually lost.
This does not mean you must take HRT forever. But it does mean that stopping HRT requires a transition plan:
Discuss bisphosphonate therapy as a bridge to maintain bone density after HRT discontinuation
Get a DEXA scan within 1-2 years of stopping to assess the rate of bone loss
Intensify weight-bearing exercise and ensure adequate calcium and vitamin D intake
Consider a gradual taper rather than abrupt cessation to reduce symptom rebound and potentially slow the rate of bone loss
For women who started HRT primarily for bone protection, the decision to stop should involve a conversation with their provider about alternative bone-protective strategies.
Pouilles JM, Tremollieres F, Ribot C. Rates of bone loss in normal women: evidence of accelerated trabecular bone loss after the menopause. Osteoporos Int. 1993;3(1):15-22. PMID: 3147906
Cauley JA, Robbins J, Chen Z, et al. Effects of estrogen plus progestin on risk of fracture and bone mineral density: the Women's Health Initiative randomized trial. JAMA. 2003;290(13):1729-1738. PMID: 14519707
Manolagas SC, O'Brien CA, Almeida M. Direct and indirect estrogen actions on osteoblasts and osteoclasts. Int J Biochem Cell Biol. 2013;45(12):2721-2726. PMID: 16831916
Davis SR, McCloud P, Strauss BJ, Burger H. Testosterone enhances estradiol's effects on postmenopausal bone density and sexuality. Maturitas. 1995;21(3):227-236. PMID: 7616872
Gambacciani M, Levancini M. Menopausal hormone therapy for the management of osteoporosis. Endocrine. 2021;73(2):294-299. PMID: 34119418
Camacho PM, Petak SM, Binkley N, et al. American Association of Clinical Endocrinologists/American College of Endocrinology clinical practice guidelines for the diagnosis and treatment of postmenopausal osteoporosis -- 2020 update. Endocr Pract. 2020;26(Suppl 1):1-46. PMID: 32427503
Davis SR, Baber RJ, Panay N, et al. Global Consensus Position Statement on the Use of Testosterone Therapy for Women. J Sex Med. 2019;16(9):1331-1337. PMID: 31488288
U.S. Preventive Services Task Force. Screening for Osteoporosis to Prevent Fractures: USPSTF Recommendation Statement. JAMA. 2025;333(6):498-505. PMID: 39808425
Frequently Asked Questions
Does HRT actually prevent osteoporosis?
Yes. The Women's Health Initiative trial showed that combined estrogen-progestin therapy reduced fracture risk by 24% across all sites and increased bone mineral density by 3.7% at the hip and 4.5% at the spine over 5 years. Estrogen-only therapy showed similar fracture protection.
When should I start HRT for bone protection?
The strongest bone protection comes from starting HRT within the first few years of menopause, when bone loss is fastest. Women lose bone most rapidly in the 5-7 years after their final menstrual period. Starting early preserves more bone than trying to rebuild it later.
Is HRT better than bisphosphonates for bone density?
Both are effective, but they work differently. HRT addresses the root cause of menopausal bone loss (estrogen deficiency) and provides systemic benefits beyond bone. Bisphosphonates are bone-specific and preferred for women over 60 or those who cannot take HRT. For recently menopausal women with vasomotor symptoms, HRT is often the better first choice.
Does testosterone help with bone density in women?
Yes. Research shows that adding testosterone to estrogen therapy produces greater bone density gains than estrogen alone, particularly at the hip and spine. Testosterone stimulates osteoblasts (bone-building cells) through androgen receptors that estrogen does not activate.
How often should I get a DEXA scan during menopause?
The USPSTF recommends screening all women at age 65. Postmenopausal women under 65 with risk factors (low body weight, family history, smoking, early menopause) should get a baseline DEXA earlier. If you are on HRT for bone protection, repeat DEXA every 2 years to monitor response.
Will I lose bone density if I stop HRT?
Yes. Bone loss resumes and accelerates after stopping HRT. Studies show that fracture protection from HRT diminishes within 2-3 years of discontinuation. If you stop HRT, discuss alternative bone protection strategies with your provider.